Adrenocortical Carcinoma Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Adrenocortical Carcinoma
Adrenocortical carcinoma is a rare disease in which malignant (cancer) cells form in the outer layer of the adrenal gland.
There are two adrenal glands. The adrenal glands are small and shaped like a triangle. One adrenal gland sits on top of each kidney. Each adrenal gland has two parts. The outer layer of the adrenal gland is the adrenal cortex. The center of the adrenal gland is the adrenal medulla. 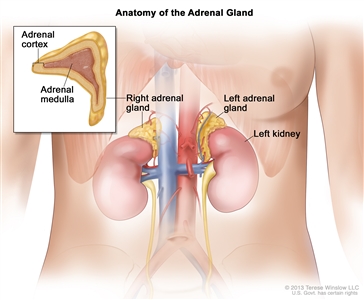
Anatomy of the adrenal gland. There are two adrenal glands, one on top of each kidney. The outer part of each gland is the adrenal cortex and the inner part is the adrenal medulla.
The adrenal cortex makes important hormones that:
- Balance the water and salt in the body.
- Help keep blood pressure normal.
- Help control the body's use of protein, fat, and carbohydrates.
- Cause the body to have masculine or feminine characteristics.
Adrenocortical carcinoma is also called cancer of the adrenal cortex. A tumor of the adrenal cortex may be functioning (makes more hormones than normal) or nonfunctioning (does not make more hormones than normal). Most adrenocortical tumors are functioning. The hormones made by functioning tumors may cause certain signs or symptoms of disease.
The adrenal medulla makes hormones that help the body react to stress. Cancer that forms in the adrenal medulla is called pheochromocytoma and is not discussed in this summary. Learn more about
Adrenocortical carcinoma and pheochromocytoma can occur in both adults and children. Treatment for children, however, is different than treatment for adults. Learn more about
Having certain genetic conditions increases the risk of adrenocortical carcinoma.
Anything that increases a person's risk of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop adrenocortical carcinoma, and it will develop in some people who don't have any known risk factors. Talk with your doctor if you think you may be at risk.
Risk factors for adrenocortical carcinoma include having the following hereditary diseases:
- Li-Fraumeni syndrome.
- Beckwith-Wiedemann syndrome.
- Carney complex.
Symptoms of adrenocortical carcinoma include pain in the abdomen.
These and other signs and symptoms may be caused by adrenocortical carcinoma:
- A lump in the abdomen.
- Pain the abdomen or back.
- A feeling of fullness in the abdomen.
A nonfunctioning adrenocortical tumor may not cause signs or symptoms in the early stages.
A functioning adrenocortical tumor makes too much of one of the following hormones:
- Cortisol.
- Aldosterone.
- Testosterone.
- Estrogen.
Too much cortisol may cause:
- Weight gain in the face, neck, and trunk of the body and thin arms and legs.
- Growth of fine hair on the face, upper back, or arms.
- A round, red, full face.
- A lump of fat on the back of the neck.
- A deepening of the voice and swelling of the sex organs or breasts in both males and females.
- Muscle weakness.
- High blood sugar.
- High blood pressure.
Too much aldosterone may cause:
- High blood pressure.
- Muscle weakness or cramps.
- Frequent urination.
- Feeling thirsty.
Too much testosterone (in women) may cause:
- Growth of fine hair on the face, upper back, or arms.
- Acne.
- Balding.
- A deepening of the voice.
- No menstrual periods.
Men who make too much testosterone do not usually have signs or symptoms.
Too much estrogen (in women) may cause:
- Irregular menstrual periods in women who have not gone through menopause.
- Vaginal bleeding in women who have gone through menopause.
- Weight gain.
Too much estrogen (in men) may cause:
- Growth of breast tissue.
- Lower sex drive.
- Impotence.
These and other signs and symptoms may be caused by adrenocortical carcinoma or by other conditions. Check with your doctor if you have any of these problems.
Imaging studies and tests that examine the blood and urine are used to diagnose adrenocortical carcinoma.
The tests and procedures used to diagnose adrenocortical carcinoma depend on the patient's signs and symptoms. In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Twenty-four-hour urine test: A test in which urine is collected for 24 hours to measure the amounts of cortisol or 17-ketosteroids. A higher-than-normal amount of these in the urine may be a sign of disease in the adrenal cortex.
- Low-dose dexamethasone suppression test: A test in which one or more small doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol.
- High-dose dexamethasone suppression test: A test in which one or more high doses of dexamethasone are given. The level of cortisol is checked from a sample of blood or from urine that is collected for three days. This test is done to check if the adrenal gland is making too much cortisol or if the pituitary gland is telling the adrenal glands to make too much cortisol.
- Blood chemistry study: A procedure in which a blood sample is checked to measure the amounts of certain substances, such as potassium or sodium, released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI). An MRI of the abdomen is done to diagnose adrenocortical carcinoma.
- Adrenal angiography: A procedure to look at the arteries and the flow of blood near the adrenal glands. A contrast dye is injected into the adrenal arteries. As the dye moves through the arteries, a series of x-rays are taken to see if any arteries are blocked.
- Adrenal venography: A procedure to look at the adrenal veins and the flow of blood near the adrenal glands. A contrast dye is injected into an adrenal vein. As the contrast dye moves through the veins, a series of x-rays are taken to see if any veins are blocked. A catheter (very thin tube) may be inserted into the vein to take a blood sample, which is checked for abnormal hormone levels.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- MIBG scan: A very small amount of radioactive material called MIBG is injected into a vein and travels through the bloodstream. Adrenal gland cells take up the radioactive material and are detected by a device that measures radiation. This scan is done to tell the difference between adrenocortical carcinoma and pheochromocytoma.
- Biopsy: The removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. The sample may be taken using a thin needle, called a fine-needle aspiration (FNA) biopsy or a wider needle, called a core biopsy.
Certain factors affect the prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on:
- The stage of the cancer (the size of the tumor and whether it is in the adrenal gland only or has spread to other places in the body).
- Whether the tumor can be completely removed in surgery.
- Whether the cancer has been treated in the past.
- The patient's general health.
- The grade of tumor cells (how different they look from normal cells under a microscope).
Adrenocortical carcinoma may be cured if treated at an early stage.
Stages of Adrenocortical Carcinoma
After adrenocortical carcinoma has been diagnosed, tests are done to find out if cancer cells have spread within the adrenal gland or to other parts of the body.
The process used to find out if cancer has spread within the adrenal gland or to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment. The following tests and procedures may be used in the staging process:
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the abdomen or chest, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- MRI (magnetic resonance imaging) with gadolinium: A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the abdomen. A substance called gadolinium may be injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs, such as the vena cava, and make echoes. The echoes form a picture of body tissues called a sonogram.
- Adrenalectomy: A procedure to remove the affected adrenal gland. A tissue sample is viewed under a microscope by a pathologist to check for signs of cancer.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if adrenocortical carcinoma spreads to the lung, the cancer cells in the lung are actually adrenocortical carcinoma cells. The disease is metastatic adrenocortical carcinoma, not lung cancer.
The following stages are used for adrenocortical carcinoma:
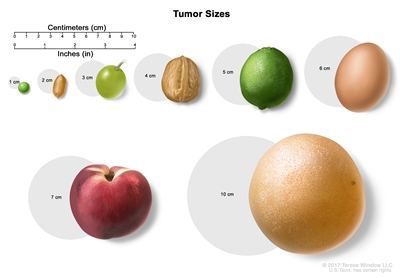
Tumor sizes are often measured in centimeters (cm) or inches. Common food items that can be used to show tumor size in cm include: a pea (1 cm), a peanut (2 cm), a grape (3 cm), a walnut (4 cm), a lime (5 cm or 2 inches), an egg (6 cm), a peach (7 cm), and a grapefruit (10 cm or 4 inches).
Stage I
In stage I, the tumor is 5 centimeters or smaller and is found in the adrenal gland only.
Stage II
In stage II, the tumor is larger than 5 centimeters and is found in the adrenal gland only.
Stage III
In stage III, the tumor is any size and has spread:
- to nearby lymph nodes; or
- to nearby tissues or organs (kidney, diaphragm, pancreas, spleen, or liver) or to large blood vessels (renal vein or vena cava) and may have spread to nearby lymph nodes.
Stage IV
In stage IV, the tumor is any size, may have spread to nearby lymph nodes, and has spread to other parts of the body, such as the lung, bone, or peritoneum.
Adrenocortical carcinoma can recur (come back) after it has been treated.
The cancer may come back in the adrenal cortex or in other parts of the body.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.