Adult Primary Liver Cancer Treatment (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Adult Primary Liver Cancer
Liver cancer includes two major types: hepatocellular carcinoma (HCC) and intrahepatic bile duct cancer. For information about bile duct cancer, see Bile Duct Cancer (Cholangiocarcinoma) Treatment. For more information about other, less common types of liver cancer, see the Cellular Classification of Adult Primary Liver Cancer section.
Incidence and Mortality
Estimated new cases and deaths from liver and intrahepatic bile duct cancer in the United States in 2023:[
- New cases: 41,210.
- Deaths: 29,380.
HCC is relatively uncommon in the United States, although its incidence is rising, principally in relation to the spread of hepatitis C virus infection.[
Anatomy
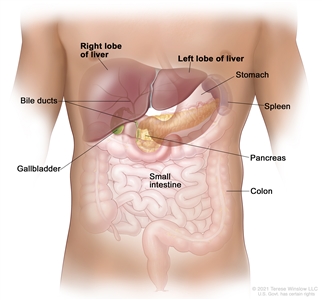
Anatomy of the liver. The liver is in the upper abdomen near the stomach, intestines, gallbladder, and pancreas. The liver has a right lobe and a left lobe. Each lobe is divided into two sections (not shown).
Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for liver (hepatocellular) cancer include the following:
- Chronic and/or persistent infection with hepatitis B and/or hepatitis C.[
4 ,5 ,6 ,7 ] - Cirrhosis.[
5 ,7 ,8 ] - Heavy alcohol use.[
6 ,8 ,9 ] - Ingestion of foods contaminated with aflatoxin B1.[
10 ,11 ,12 ,13 ] - Nonalcoholic steatohepatitis (NASH).[
14 ,15 ,16 ,17 ] - Tobacco use.[
18 ,19 ,20 ] - Certain inherited or rare disorders that include the following:
- Hereditary hemochromatosis.[
7 ,10 ] - Alpha-1 antitrypsin deficiency.[
21 ] - Glycogen storage disease.[
10 ] - Porphyria cutanea tarda.[
10 ] - Wilson disease.[
10 ,22 ,23 ]
- Hereditary hemochromatosis.[
For more information, see Liver (Hepatocellular) Cancer Prevention.
Screening
For more information, see Liver (Hepatocellular) Cancer Screening.
Diagnostic Factors
For lesions that are smaller than 1 cm and are detected during screening in patients at high risk for HCC, further diagnostic evaluation is not required because most of these lesions will be cirrhotic lesions rather than HCC.[
For patients with liver lesions larger than 1 cm who are at risk for HCC, a diagnosis can be considered. The tests required to diagnose HCC may include imaging, biopsy, or both.
Diagnostic imaging
In patients with cirrhosis, liver disease, or other risk factors for HCC, and with lesions greater than 1 cm, triple-phase, contrast-enhanced studies (dynamic computed tomography [CT] or magnetic resonance imaging [MRI]) can be used to establish a diagnosis of HCC.[
A triple-phase CT or MRI assesses the entire liver in distinct phases of perfusion. Following the controlled administration of intravenous contrast media, the arterial and venous phases of perfusion are imaged.
During the arterial phase of the study, HCC enhances more intensely than the surrounding liver because the arterial blood in the liver is diluted by venous blood that does not contain contrast, whereas the HCC contains only arterial blood. In the venous phase, the HCC enhances less than the surrounding liver (which is referred to as the venous washout of HCC), because the arterial blood flowing through the lesion no longer contains contrast; however, the portal blood in the liver now contains contrast.
The presence of arterial uptake followed by washout in a single dynamic study is highly specific (95%–100%) for HCC of 1 to 3 cm in diameter and virtually diagnostic of HCC.[
However, if a first imaging modality, such as a contrast-enhanced CT or MRI, is not conclusive, sequential imaging with a different modality can improve sensitivity for HCC detection (from 33% to 41% for either CT or MRI to 76% for both studies when performed sequentially) without a decrease in specificity.[
If, despite the use of two imaging modalities, a lesion larger than 1 cm remains uncharacterized in a patient at high risk for HCC (i.e., with no or only one classic enhancement pattern), a liver biopsy can be considered.[
Liver biopsy
A liver biopsy may be performed when a diagnosis of HCC is not established by a dynamic imaging modality (three-phase CT or MRI) for liver lesions 1 cm or larger in high-risk patients.
Alpha-fetoprotein (AFP) levels
AFP is insufficiently sensitive or specific for use as a diagnostic assay. AFP can be elevated in intrahepatic cholangiocarcinoma and in some cases in which there are metastases from colon cancer. Finding a mass in the liver of a patient with an elevated AFP does not automatically indicate HCC. However, if the AFP level is high, it can be used to monitor for recurrence.
Prognosis
The natural course of early tumors is poorly known because most HCC patients are treated. However, older reports have described 3-year survival rates of 13% to 21% without any specific treatment.[
Liver transplantation, surgical resection, and ablation offer high rates of complete responses and a potential for cure in patients with early HCC.[
The natural course of advanced-stage HCC is better known. Untreated patients with advanced disease usually survive less than 6 months.[
Unlike most patients with solid tumors, the prognosis of patients with HCC is affected by the tumor stage at presentation and by the underlying liver function. The following prognostic factors guide the selection of treatment:
- Anatomic extension of the tumor (i.e., tumor size, number of lesions, presence of vascular invasion, and extrahepatic spread).
- Performance status.
- Functional hepatic reserve based on the Child-Pugh score.[
36 ,38 ,39 ]
References:
- American Cancer Society: Cancer Facts and Figures 2023. American Cancer Society, 2023. Available online. Last accessed January 13, 2023.
- Altekruse SF, McGlynn KA, Reichman ME: Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol 27 (9): 1485-91, 2009.
- Forner A, Llovet JM, Bruix J: Hepatocellular carcinoma. Lancet 379 (9822): 1245-55, 2012.
- Bosetti C, Turati F, La Vecchia C: Hepatocellular carcinoma epidemiology. Best Pract Res Clin Gastroenterol 28 (5): 753-70, 2014.
- El-Serag HB: Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 142 (6): 1264-1273.e1, 2012.
- El-Serag HB, Kanwal F: Epidemiology of hepatocellular carcinoma in the United States: where are we? Where do we go? Hepatology 60 (5): 1767-75, 2014.
- Lafaro KJ, Demirjian AN, Pawlik TM: Epidemiology of hepatocellular carcinoma. Surg Oncol Clin N Am 24 (1): 1-17, 2015.
- Fattovich G, Stroffolini T, Zagni I, et al.: Hepatocellular carcinoma in cirrhosis: incidence and risk factors. Gastroenterology 127 (5 Suppl 1): S35-50, 2004.
- Grewal P, Viswanathen VA: Liver cancer and alcohol. Clin Liver Dis 16 (4): 839-50, 2012.
- London WT, McGlynn K: Liver cancer. In: Schottenfeld D, Fraumeni JF Jr, eds.: Cancer Epidemiology and Prevention. 3rd ed. Oxford University Press, 2006, pp 763-86.
- McGlynn KA, Petrick JL, London WT: Global epidemiology of hepatocellular carcinoma: an emphasis on demographic and regional variability. Clin Liver Dis 19 (2): 223-38, 2015.
- Liu Y, Wu F: Global burden of aflatoxin-induced hepatocellular carcinoma: a risk assessment. Environ Health Perspect 118 (6): 818-24, 2010.
- Chen JG, Egner PA, Ng D, et al.: Reduced aflatoxin exposure presages decline in liver cancer mortality in an endemic region of China. Cancer Prev Res (Phila) 6 (10): 1038-45, 2013.
- Baffy G, Brunt EM, Caldwell SH: Hepatocellular carcinoma in non-alcoholic fatty liver disease: an emerging menace. J Hepatol 56 (6): 1384-91, 2012.
- Diehl AM, Day C: Cause, Pathogenesis, and Treatment of Nonalcoholic Steatohepatitis. N Engl J Med 377 (21): 2063-2072, 2017.
- White DL, Kanwal F, El-Serag HB: Association between nonalcoholic fatty liver disease and risk for hepatocellular cancer, based on systematic review. Clin Gastroenterol Hepatol 10 (12): 1342-1359.e2, 2012.
- Ascha MS, Hanouneh IA, Lopez R, et al.: The incidence and risk factors of hepatocellular carcinoma in patients with nonalcoholic steatohepatitis. Hepatology 51 (6): 1972-8, 2010.
- Chuang SC, Lee YC, Hashibe M, et al.: Interaction between cigarette smoking and hepatitis B and C virus infection on the risk of liver cancer: a meta-analysis. Cancer Epidemiol Biomarkers Prev 19 (5): 1261-8, 2010.
- Lee YC, Cohet C, Yang YC, et al.: Meta-analysis of epidemiologic studies on cigarette smoking and liver cancer. Int J Epidemiol 38 (6): 1497-511, 2009.
- Koh WP, Robien K, Wang R, et al.: Smoking as an independent risk factor for hepatocellular carcinoma: the Singapore Chinese Health Study. Br J Cancer 105 (9): 1430-5, 2011.
- Lomas DA, Evans DL, Finch JT, et al.: The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature 357 (6379): 605-7, 1992.
- Huster D: Wilson disease. Best Pract Res Clin Gastroenterol 24 (5): 531-9, 2010.
- Pfeiffenberger J, Mogler C, Gotthardt DN, et al.: Hepatobiliary malignancies in Wilson disease. Liver Int 35 (5): 1615-22, 2015.
- Furuya K, Nakamura M, Yamamoto Y, et al.: Macroregenerative nodule of the liver. A clinicopathologic study of 345 autopsy cases of chronic liver disease. Cancer 61 (1): 99-105, 1988.
- Brunello F, Cantamessa A, Gaia S, et al.: Radiofrequency ablation: technical and clinical long-term outcomes for single hepatocellular carcinoma up to 30 mm. Eur J Gastroenterol Hepatol 25 (7): 842-9, 2013.
- Leoni S, Piscaglia F, Golfieri R, et al.: The impact of vascular and nonvascular findings on the noninvasive diagnosis of small hepatocellular carcinoma based on the EASL and AASLD criteria. Am J Gastroenterol 105 (3): 599-609, 2010.
- Khalili K, Kim TK, Jang HJ, et al.: Optimization of imaging diagnosis of 1-2 cm hepatocellular carcinoma: an analysis of diagnostic performance and resource utilization. J Hepatol 54 (4): 723-8, 2011.
- Sangiovanni A, Manini MA, Iavarone M, et al.: The diagnostic and economic impact of contrast imaging techniques in the diagnosis of small hepatocellular carcinoma in cirrhosis. Gut 59 (5): 638-44, 2010.
- Bruix J, Sherman M; American Association for the Study of Liver Diseases: Management of hepatocellular carcinoma: an update. Hepatology 53 (3): 1020-2, 2011.
- Khalili K, Kim TK, Jang HJ, et al.: Implementation of AASLD hepatocellular carcinoma practice guidelines in North America: two years of experience. [Abstract] Hepatology 48 (Suppl 1): A-128, 362A, 2008.
- Barbara L, Benzi G, Gaiani S, et al.: Natural history of small untreated hepatocellular carcinoma in cirrhosis: a multivariate analysis of prognostic factors of tumor growth rate and patient survival. Hepatology 16 (1): 132-7, 1992.
- Ebara M, Ohto M, Shinagawa T, et al.: Natural history of minute hepatocellular carcinoma smaller than three centimeters complicating cirrhosis. A study in 22 patients. Gastroenterology 90 (2): 289-98, 1986.
- Shah SA, Smith JK, Li Y, et al.: Underutilization of therapy for hepatocellular carcinoma in the medicare population. Cancer 117 (5): 1019-26, 2011.
- Sonnenday CJ, Dimick JB, Schulick RD, et al.: Racial and geographic disparities in the utilization of surgical therapy for hepatocellular carcinoma. J Gastrointest Surg 11 (12): 1636-46; discussion 1646, 2007.
- Dhir M, Lyden ER, Smith LM, et al.: Comparison of outcomes of transplantation and resection in patients with early hepatocellular carcinoma: a meta-analysis. HPB (Oxford) 14 (9): 635-45, 2012.
- Okuda K, Ohtsuki T, Obata H, et al.: Natural history of hepatocellular carcinoma and prognosis in relation to treatment. Study of 850 patients. Cancer 56 (4): 918-28, 1985.
- Llovet JM, Bruix J: Systematic review of randomized trials for unresectable hepatocellular carcinoma: Chemoembolization improves survival. Hepatology 37 (2): 429-42, 2003.
- Llovet JM, Brú C, Bruix J: Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis 19 (3): 329-38, 1999.
- A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients: the Cancer of the Liver Italian Program (CLIP) investigators. Hepatology 28 (3): 751-5, 1998.
This information does not replace the advice of a doctor. Healthwise, Incorporated, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Healthwise, Incorporated.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.