Bladder Cancer Treatment: Treatment - Patient Information [NCI]
What Is Bladder Cancer?
Bladder cancer occurs when cells in the bladder start to grow without control. The bladder is a hollow, balloon-shaped organ in the lower part of the abdomen that stores urine.
The bladder has a muscular wall that allows it to get larger to store urine made by the kidneys and to shrink to squeeze urine out of the body. There are two kidneys, one on each side of the backbone, above the waist. The bladder and kidneys work together to remove toxins and wastes from your body through urine:
- Tiny tubules in the kidneys filter and clean the blood.
- These tubules take out waste products and make urine.
- The urine passes from each kidney through a long tube called a ureter into the bladder.
- The bladder holds the urine until it passes through a tube called the urethra and leaves the body.
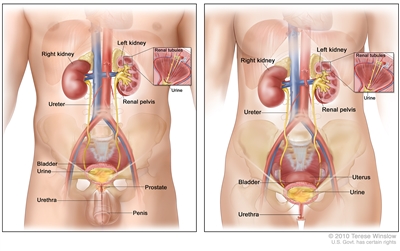
Anatomy of the male urinary system (left panel) and female urinary system (right panel) showing the kidneys, ureters, bladder, and urethra. The inside of the left kidney shows the renal pelvis. An inset shows the renal tubules and urine. Also shown are the prostate and penis (left panel) and the uterus (right panel). Urine is made in the renal tubules and collects in the renal pelvis of each kidney. The urine flows from the kidneys through the ureters to the bladder. The urine is stored in the bladder until it leaves the body through the urethra.
Types of bladder cancer
Urothelial carcinoma (also called transitional cell carcinoma) is cancer that begins in the urothelial cells, which line the urethra, bladder, ureters, renal pelvis, and some other organs. Almost all bladder cancers are urothelial carcinomas.
Urothelial cells are also called transitional cells because they change shape. These cells are able to stretch when the bladder is full of urine and shrink when it is emptied.
Other types of bladder cancer are rare:
- Squamous cell carcinoma is cancer that begins in squamous cells (thin, flat cells lining the inside of the bladder). This type of cancer may form after long-term irritation or infection with a tropical parasite called schistosomiasis, which is common in Africa and the Middle East but rare in the United States. When chronic irritation occurs, transitional cells that line the bladder can gradually change to squamous cells.
- Adenocarcinoma is cancer that begins in glandular cells that are found in the lining of the bladder. Glandular cells in the bladder make mucus and other substances.
- Small cell carcinoma of the bladder is cancer that begins in neuroendocrine cells (nerve-like cells that release hormones into the blood in response to a signal from the nervous system).
There are other ways to describe bladder cancer:
- Non-muscle-invasive bladder cancer is cancer that has not reached the muscle wall of the bladder. Most bladder cancers are non-muscle-invasive.
- Muscle-invasive bladder cancer is cancer that has spread through the lining of the bladder and into the muscle wall of the bladder or beyond it.
Learn more about bladder cancer
Many bladder cancer symptoms are also seen with other less serious conditions. These are the warning signs you shouldn't ignore.
Using tobacco, especially smoking cigarettes, is a major risk factor for bladder cancer. Learn about tobacco use and other risk factors for bladder cancer and what you can do to lower your risk.
Learn about bladder cancer screening tests for people at high risk.
Learn about the tests that are used to diagnose and stage bladder cancer.
Learn about bladder cancer survival rates and why this statistic doesn't predict exactly what will happen to you.
Stage refers to the extent of your cancer, such as how large the tumor is and if it has spread. Learn about bladder cancer stages, an important factor in deciding your treatment plan.
Learn about the different ways bladder cancer can be treated.
Coping with bladder cancer and the side effects of treatment can feel overwhelming. Learn about resources to help you cope and gain a sense of control.
Childhood bladder cancer is a very rare type of cancer that forms in the tissues of the bladder. Learn about the symptoms of bladder cancer in children, and how it is diagnosed and treated.
Bladder Cancer Diagnosis
If you have symptoms or lab test results that suggest bladder cancer, your doctor will need to find out if they're due to cancer or another condition. Your doctor may
- ask about your personal and family medical history to learn more about your symptoms and possible risk factors for bladder cancer
- ask for a sample of your urine so it can be checked in the lab for blood, abnormal cells, or infection
- do a physical exam, which for women, may include a pelvic exam, to check for signs of cancer
Depending on your symptoms, medical history, and results of your urine lab tests and physical exam, your doctor may recommend more tests to find out if you have bladder cancer, and if so, its extent (stage).
Tests to diagnose bladder cancer
The following tests and procedures are used to diagnose bladder cancer. The results will also help you and your doctor plan treatment.
Cystoscopy
Cystoscopy is a procedure in which the doctor looks inside the bladder and urethra (the tube that carries urine out of your body) to check for abnormal areas. A cystoscope is slowly inserted through the urethra into the bladder to allow the doctor to see inside. A cystoscope is a thin, tube-like instrument with a light and a lens for viewing. It may also have a tool to remove very small bladder tumors or tissue samples for biopsy. Cystoscopy helps to diagnose, and sometimes treat, bladder cancer and other conditions.
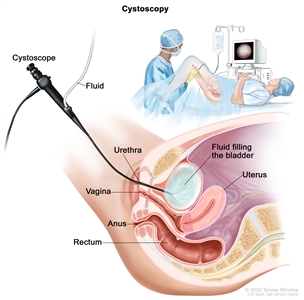
Cystoscopy. A cystoscope (a thin, tube-like instrument with a light and a lens for viewing) is inserted through the urethra into the bladder. Fluid is used to fill the bladder. The doctor looks at an image of the inner wall of the bladder on a computer monitor to check for abnormal areas.
Biopsy
A biopsy is usually done during a cystoscopy procedure. Biopsy is a procedure in which a sample of cells or tissue is removed from the bladder so that a pathologist can view it under a microscope to check for signs of cancer. It may be possible to remove the entire tumor at the time of the biopsy.
Talk with your doctor to learn what to expect during and after your cystoscopy and biopsy. Some people have blood in the urine or discomfort and a burning sensation while urinating for a day or two.
To learn about the type of information that can be found in a pathologist's report about the cells or tissue removed during a biopsy, see
Computed tomography (CT) urogram or intravenous pyelogram (IVP)
CT urogram is a test that takes a CT scan of the urinary tract using a contrast dye injected into a vein. To begin the procedure, a CT machine takes a series of detailed pictures of the kidneys. The contrast dye is then injected, and another CT scan of the kidneys, bladder, and ureters is done. About 10 minutes later, a final scan is taken as the contrast dye drains from the kidneys into the bladder. CT urogram also captures detailed pictures of nearby bones, soft tissues, and blood vessels. This allows the doctor to see how well your urinary tract is working and to check for signs of disease.
IVP is an x-ray imaging test of your urinary tract. After a contrast dye is injected into a vein, a series of x-ray pictures of the kidneys, ureters, and bladder are taken to find out if cancer is present in these organs. As the contrast dye moves through the kidneys, ureters, and bladder, more x-ray pictures are taken at specific times. This allows your doctor to see how well your urinary tract is working and to check for signs of disease.
Urine tumor marker test
Urinary tumor markers are substances found in the urine that are either made by bladder cancer cells or that the body makes in response to bladder cancer. For this test, a sample of urine is checked in the lab to detect the presence of these substances. Urine tumor marker tests may be used to help diagnose some types of bladder cancer.
Tests to stage bladder cancer
If you're diagnosed with bladder cancer, you will be referred to a urologic oncologist. This is a doctor who specializes in diagnosing and treating cancers of the male and female urinary tract and the male reproductive organs. They will recommend tests to determine the extent of cancer. Sometimes the cancer is only in the bladder. Or, it may have spread from the bladder to other parts of the body. The process of learning the extent of cancer in the body is called staging. It is important to know the stage of the bladder cancer to plan treatment.
For information about a specific stage of bladder cancer, see
The following imaging tests may be used to determine the bladder cancer stage.
Computed tomography (CT) scan
A CT scan uses a computer linked to an x-ray machine to make a series of detailed x-ray pictures of areas inside the body from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly.
Magnetic resonance imaging (MRI)
MRI uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the bladder. This procedure is also called nuclear magnetic resonance imaging. Images may be taken at three different times after the dye is injected, to get the best picture of abnormal areas in the bladder. This is called triple-phase MRI.
Chest x-ray
A chest x-ray is an x-ray of the organs and bones inside the chest. An x-ray is a type of high-energy radiation that can go through the body and onto film, making a picture of areas inside the chest.
Bone scan
A bone scan is a procedure that checks to see if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner.
Getting a second opinion
Some people may want to get a second opinion to confirm their bladder cancer diagnosis and treatment plan. If you choose to seek a second opinion, you will need to get important medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the pathology report, slides, and scans before giving a recommendation. The doctor who gives the second opinion may agree with your first doctor, suggest changes or another approach, or provide more information about your cancer.
To learn more about choosing a doctor and getting a second opinion, see
Bladder Cancer Stages
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. It's important to know the stage of bladder cancer to plan treatment.
There are several different staging systems for cancer. Bladder cancer is usually staged using the TNM staging system. Your cancer may be described by this staging system in your pathology report. Based on the TNM results, a stage is assigned to your cancer, such as stage I, stage II, stage III, or stage IV (may also be written as stage 1, stage 2, stage 3, or stage 4). When talking with you about your cancer, your doctor may describe it as one of these stages.
Learn more about
Learn about the
Stage 0 (noninvasive papillary carcinoma and carcinoma in situ)
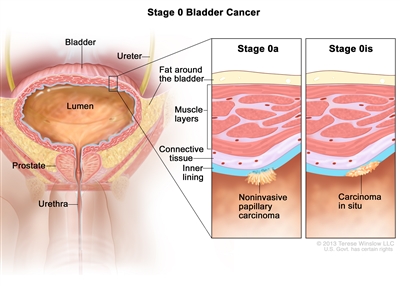
Stage 0 bladder cancer (noninvasive bladder cancer). Cancer cells are found in tissue lining the inside of the bladder but have not invaded into the bladder wall. Stage 0a (also called noninvasive papillary carcinoma) may look like long, thin growths extending into the bladder lumen (the space where urine collects). Stage 0is (also called carcinoma in situ) is a flat tumor on the tissue lining the inside of the bladder.
Stage 0 refers to noninvasive bladder cancer. This means that cancer cells are found in tissue lining the inside of the bladder but have not invaded the bladder wall. Stage 0 is divided into stages 0a and 0is, depending on the type of tumor:
- Stage 0a is also called noninvasive papillary carcinoma, which may look like long, thin growths extending into the bladder lumen (the space where urine collects). Stage 0a can be low grade or high grade, depending on how abnormal the cells look under the microscope (see the section on
Bladder cancer grade ). - Stage 0is is also called carcinoma in situ, which is a flat tumor on the tissue lining the inside of the bladder. Stage 0is is always high grade (see the section on
Bladder cancer grade ).
Learn about treatment for
Stage I bladder cancer
Stage I is a form of non-muscle-invasive bladder cancer that has spread into the connective tissue but has not reached the muscle layers of the bladder.

Stage I bladder cancer (non-muscle-invasive bladder cancer). Cancer has spread into the connective tissue but has not reached the muscle layers of the bladder.
Learn about treatment for
Stage II bladder cancer
Stage II may also be described as muscle-invasive bladder cancer. In stage II, cancer has spread through the connective tissue into the muscle layers of the bladder.

Stage II bladder cancer (muscle-invasive bladder cancer). Cancer has spread through the connective tissue into the muscle layers of the bladder.
Learn about treatment for
Stage III bladder cancer
Stage III may also be described as locally advanced bladder cancer. Stage III is divided into stages IIIA and IIIB.
- In stage IIIA
- cancer has grown all the way through the bladder muscles and bladder wall into the layer of fat surrounding the bladder and may have spread to the reproductive organs (prostate, seminal vesicles, uterus, or vagina) but has not spread to lymph nodes; or
- cancer has spread to one lymph node in the pelvis that is not near the major arteries in the pelvis, called the common iliac arteries.

Stage IIIA bladder cancer. Cancer (a) has grown all the way through the bladder muscles and bladder wall into the layer of fat around the bladder and may have spread to the prostate and/or seminal vesicles in men or the uterus and/or vagina in women but has not spread to lymph nodes; or (b) has spread to one lymph node in the pelvis that is not near the common iliac arteries.
- In stage IIIB, cancer has spread to more than one lymph node in the pelvis that is not near the common iliac arteries or to at least one lymph node that is near the common iliac arteries.
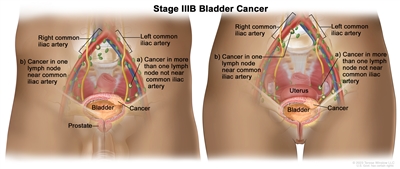
Stage IIIB bladder cancer. Cancer has spread to (a) more than one lymph node in the pelvis that is not near the common iliac arteries; or (b) at least one lymph node that is near the common iliac arteries.
Learn about treatment for
Stage IV bladder cancer
Stage IV is divided into stages IVA and IVB.
- In stage IVA
- cancer has spread to the abdominal wall or pelvic wall; or
- cancer has spread to lymph nodes that are above the major arteries in the pelvis, called the common iliac arteries.
- In stage IVB, cancer has spread to other parts of the body, such as the lung, bone, or liver.
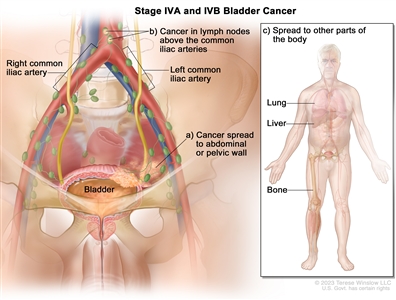
Stage IVA and IVB bladder cancer. In stage IVA, cancer has spread to (a) the abdominal or pelvic wall; or (b) lymph nodes above the common iliac arteries. In stage IVB, cancer has spread to (c) other parts of the body, such as the lung, liver, or bone.
Stage IV bladder cancer is also called metastatic bladder cancer. Metastatic cancer happens when cancer cells travel through the lymphatic system or blood and form tumors in other parts of the body. The metastatic tumor is the same type of cancer as the primary tumor. For example, if bladder cancer spreads to the lung, the cancer cells in the lung are actually bladder cancer cells. The disease is called metastatic bladder cancer, not lung cancer. Learn more in
Learn about treatment for
Bladder cancer grade
Cancer grade describes how abnormal the bladder cancer cells look under a microscope and how quickly the cancer cells are likely to grow and spread. Your doctor uses grade and other factors about your cancer, such as its stage, to form a treatment plan and in some cases, to estimate your prognosis.
- Low-grade bladder cancer cells look more like normal cells and tend to grow and spread more slowly than high-grade cancer cells.
- High-grade bladder cancer tends to grow and spread more quickly than low-grade bladder cancer. High-grade cancers usually have a worse prognosis than low-grade cancers and may need treatment right away or treatment that is more aggressive
To learn more, see
Recurrent bladder cancer
Recurrent bladder cancer is cancer that has recurred (come back) after it has been treated. Bladder cancer tends to recur after treatment, even when it is noninvasive at the time of diagnosis. Low-grade bladder cancer mainly recurs in the bladder lining. High-grade bladder cancer is more likely to have spread to the muscle layers or other parts of the body when it recurs. Tests will be done to help determine where the cancer has returned in your body, if it has spread, and how far. The type of treatment that you have for recurrent bladder cancer will depend on where it has come back.
Learn more in
Learn about treatment for
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.