Bladder Cancer Treatment (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Bladder Cancer
Incidence and Mortality
Bladder cancer is the sixth most common cancer in the United States after breast cancer, prostate cancer, lung cancer, colon cancer, and melanoma. It is the fourth most common cancer in men and the twelfth most common cancer in women. Of the approximately 84,000 new cases annually, about 65,000 are in men and about 19,000 are in women. Of the roughly 17,000 annual deaths, more than 12,000 are in men and fewer than 5,000 are in women. The reasons for this disparity between the sexes are not well understood.[
Estimated new cases and deaths from bladder cancer in the United States in 2025:[
- New cases: 84,870.
- Deaths: 17,420.
Anatomy
The urinary tract consists of the kidneys, the ureters, the bladder, and the urethra. The urinary tract is lined with transitional cell urothelium from the renal pelvis to the proximal urethra. Transitional cell carcinoma (also known as urothelial carcinoma) can develop anywhere along this pathway.
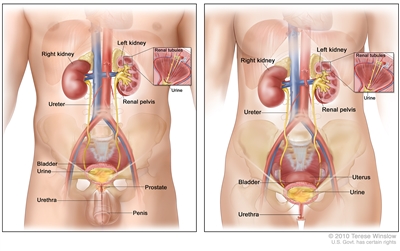
Anatomy of the male urinary system (left panel) and female urinary system (right panel) showing the kidneys, ureters, bladder, and urethra. The inside of the left kidney shows the renal pelvis. An inset shows the renal tubules and urine. Also shown are the prostate and penis (left panel) and the uterus (right panel). Urine is made in the renal tubules and collects in the renal pelvis of each kidney. The urine flows from the kidneys through the ureters to the bladder. The urine is stored in the bladder until it leaves the body through the urethra.
Histopathology
Under normal conditions, the bladder, the lower part of the kidneys (the renal pelvises), the ureters, and the proximal urethra are lined with a specialized mucous membrane referred to as transitional epithelium (also called urothelium). Most cancers that form in these tissues are transitional cell carcinomas (also called urothelial carcinomas) that derive from transitional epithelium. For more information, see
Transitional cell carcinoma of the bladder can be low-grade or high-grade:
- Low-grade bladder cancer often recurs in the bladder after treatment but rarely invades the muscular wall of the bladder or spreads to other parts of the body. Patients rarely die of low-grade bladder cancer.
- High-grade bladder cancer commonly recurs in the bladder and has a strong tendency to invade the muscular wall of the bladder and spread to other parts of the body. High-grade bladder cancer is treated more aggressively than low-grade bladder cancer and is much more likely to cause death. Almost all deaths from bladder cancer result from high-grade disease.
Bladder cancer is also divided into muscle-invasive and nonmuscle-invasive disease, based on invasion of the muscularis propria (also known as the detrusor muscle), which is the thick muscle deep in the bladder wall.
- Muscle-invasive disease is much more likely to spread to other parts of the body and is generally treated by either removing the bladder or treating the bladder with radiation and chemotherapy. As noted above, high-grade cancers are much more likely to be muscle-invasive than low-grade cancers. Thus, muscle-invasive cancers are generally treated more aggressively than nonmuscle-invasive cancers.
- Nonmuscle-invasive disease can often be treated by removing the tumor(s) via a transurethral approach. Sometimes chemotherapy or other treatments are introduced into the bladder with a catheter to help fight the cancer.
Under conditions of chronic inflammation, such as infection of the bladder with the Schistosoma haematobium parasite, squamous metaplasia may occur in the bladder. The incidence of squamous cell carcinomas of the bladder is higher under conditions of chronic inflammation than is otherwise seen. In addition to transitional cell carcinomas and squamous cell carcinomas, adenocarcinomas, small cell carcinomas, and sarcomas can form in the bladder. In the United States, transitional cell carcinomas represent most (>90%) bladder cancers. However, a significant number of transitional cell carcinomas have areas of squamous cell or other differentiation.
Carcinogenesis and Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for bladder cancer include:
- Use of tobacco, especially cigarettes.[
3 ] - Family history of bladder cancer.[
4 ] - Genetic variants.[
5 ,6 ,7 ]- HRAS variant (Costello syndrome, facio-cutaneous-skeletal syndrome).
- RB1 variant.
- PTEN/MMAC1 variant (Cowden syndrome).
- NAT2 slow acetylator phenotype.
- GSTM1 null phenotype.
- Occupational exposure to chemicals in processed paint, dye, metal, and petroleum products that include:
- Aluminum production (polycyclic aromatic hydrocarbons, fluorides).[
3 ] - Aminobiphenyl and its metabolites.[
3 ] - Aromatic amines, benzidine and its derivatives.[
3 ] - Certain aldehydes.[
8 ] - 2-Naphthylamine, beta-naphthylamine.[
3 ] - o-Toluidine.[
9 ]
- Aluminum production (polycyclic aromatic hydrocarbons, fluorides).[
- Treatment with cyclophosphamide, ifosfamide, or pelvic radiation for other malignancies.[
10 ,11 ,12 ] - Use of Chinese herbs: aristolochic acid extracted from species of Aristolochia fangchi.[
13 ] - Exposure to arsenic.
- Arsenic in well water.[
14 ,15 ,3 ] - Inorganic arsenic compounds (gallium arsenide).
- Arsenic in well water.[
- Exposure to chlorinated aliphatic hydrocarbons and chlorination by-products in treated water.[
16 ] - Schistosoma haematobium bladder infections (bilharzial bladder cancer).[
17 ] - Neurogenic bladder and associated use of indwelling catheters.[
18 ]
There is strong evidence linking exposure to carcinogens to bladder cancer. The most common risk factor for bladder cancer in the United States is cigarette smoking. It is estimated that cigarette smoking causes up to one-half of all bladder cancers and that smoking increases a person's risk of bladder cancer two to four times above baseline risk.[
Certain occupational exposures have also been linked to bladder cancer, and higher rates of bladder cancer have been reported in textile dye and rubber tire industries; among painters; leather workers; shoemakers; and aluminum-, iron-, and steelworkers. Specific chemicals linked to bladder carcinogenesis include beta-naphthylamine, 4-aminobiphenyl, and benzidine. Although these chemicals are now generally banned in Western countries, many other chemicals still in use are also suspected of causing bladder cancer.[
Exposure to the chemotherapy drug cyclophosphamide has also been associated with an increased risk of bladder cancer.
Chronic urinary tract infections and infection with the parasite S. haematobium have also been associated with an increased risk of bladder cancer, often squamous cell carcinomas. Chronic inflammation is thought to play a key role in carcinogenesis in these settings.
Clinical Features
Bladder cancer typically presents with gross or microscopic hematuria. Less commonly, patients may complain of urinary frequency, nocturia, and dysuria, symptoms that are more common in patients with carcinoma in situ. Patients with upper urinary tract urothelial carcinomas may present with pain resulting from obstruction by the tumor.
Urothelial carcinomas are often multifocal—the entire urothelium needs to be evaluated if a tumor is found. In patients with bladder cancer, upper urinary tract imaging is essential for staging and surveillance. This can be accomplished with ureteroscopy, retrograde pyelograms during cystoscopy, intravenous pyelograms, or computed tomography (CT) urograms. Similarly, patients with an upper urinary tract transitional cell carcinoma have a high risk of developing bladder cancer; these patients need periodic cystoscopy and surveillance of the contralateral upper urinary tract.
Diagnostics
When bladder cancer is suspected, the most useful diagnostic test is cystoscopy. Radiological studies such as CT scans or ultrasound do not have sufficient sensitivity to detect bladder cancers. Cystoscopy can be performed in a urology clinic.
If cancer is seen on cystoscopy, the patient is typically scheduled for bimanual examination under anesthesia and a repeat cystoscopy in an operating room so that transurethral resection of the tumor(s) and/or biopsies can be performed. If a high-grade cancer (including carcinoma in situ) or invasive cancer is seen, the patient is staged with a CT scan of the abdomen and pelvis (or CT urogram) and either a chest x-ray or chest CT scan. Patients with a nonhepatic elevation of alkaline phosphatase or symptoms suggestive of bone metastases undergo a bone scan.
Prognostic Factors
The major prognostic factors in carcinoma of the bladder include:
- Depth of invasion into the bladder wall.
- Pathological grade of the tumor.
- Presence versus absence of carcinoma in situ.
Among nonmuscle-invasive cancers, the following factors are also prognostic:[
- Number of tumors.
- Tumor size (e.g., >3 cm or <3 cm).
- Invasion of the lamina propria (Ta vs. T1).
- Whether the tumor is the primary tumor or a recurrence.
Most superficial tumors are well differentiated. Patients in whom superficial tumors are less differentiated, large, multiple, or associated with carcinoma in situ (Tis) in other areas of the bladder mucosa are at greatest risk of recurrence and the development of invasive cancer. These patients may be considered to have the entire urothelial surface at risk of cancer development.
Survival
Patients who die of bladder cancer almost always have disease that has metastasized from the bladder to other organs. Low-grade bladder cancers rarely grow into the muscular wall of the bladder and rarely metastasize, so patients with low-grade (grade I) bladder cancers rarely die of their cancer. Nonetheless, they may experience multiple relapses that need to be resected.
Almost all deaths from bladder cancer are among patients with high-grade disease, which has a much greater potential to invade deeply into the bladder's muscular wall and spread to other organs.
Approximately 70% to 80% of patients with newly diagnosed bladder cancer present with superficial bladder tumors (i.e., stage Ta, Tis, or T1). The prognosis of these patients depends largely on the grade of the tumor. Patients with high-grade tumors have a significant risk of dying of their cancer, even if it is not muscle-invasive.[
There are clinical trials suitable for patients with all stages of bladder cancer. Whenever possible, patients should consider clinical trials designed to improve upon standard therapy.
General information about clinical trials is also available from the
Follow-Up
Bladder cancer tends to recur, even when it is noninvasive at the time of diagnosis; therefore, standard practice is to perform surveillance of the urinary tract after a diagnosis of bladder cancer. However, no trials have been conducted to assess whether surveillance affects rates of progression, survival, or quality of life; nor have clinical trials defined an optimal surveillance schedule. Urothelial carcinomas are thought to reflect a so-called field defect, whereby the cancer emerges because of genetic variants that are widely present in the patient's bladder or entire urothelium. Thus, people who have had a bladder tumor resected often subsequently have recurrent tumors in the bladder, often in different locations from the site of the initial tumor. Similarly, but less commonly, they may have tumors appear in the upper urinary tract (i.e., in the renal pelvises or ureters).
An alternative explanation for these patterns of recurrence is that cancer cells that are disrupted when a tumor is resected may reimplant elsewhere in the urothelium. Support for this second theory is that tumors are more likely to recur downstream than upstream from the initial cancer. Upper urinary tract cancers are more likely to recur in the bladder than bladder cancers are to recur in the upper urinary tract.[
References:
- National Cancer Institute: SEER Cancer Stat Facts: Bladder Cancer. Bethesda, Md: National Cancer Institute.
Available online . Last accessed January 31, 2025. - American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025.
Available online . Last accessed January 16, 2025. - Burger M, Catto JW, Dalbagni G, et al.: Epidemiology and risk factors of urothelial bladder cancer. Eur Urol 63 (2): 234-41, 2013.
- Fraumeni JF Jr, Thomas LB: Malignant bladder tumors in a man and his three sons. JAMA 201 (7): 97-9, 1967.
- Marees T, Moll AC, Imhof SM, et al.: Risk of second malignancies in survivors of retinoblastoma: more than 40 years of follow-up. J Natl Cancer Inst 100 (24): 1771-9, 2008.
- Gallagher DJ, Feifer A, Coleman JA: Genitourinary cancer predisposition syndromes. Hematol Oncol Clin North Am 24 (5): 861-83, 2010.
- Lindor NM, McMaster ML, Lindor CJ, et al.: Concise handbook of familial cancer susceptibility syndromes - second edition. J Natl Cancer Inst Monogr (38): 1-93, 2008.
- Stadler WM: Molecular events in the initiation and progression of bladder cancer (review). Int J Oncol 3: 549-557, 1993.
- Brown T, Slack R, Rushton L, et al.: Occupational cancer in Britain. Urinary tract cancers: bladder and kidney. Br J Cancer 107 (Suppl 1): S76-84, 2012.
- Nieder AM, Porter MP, Soloway MS: Radiation therapy for prostate cancer increases subsequent risk of bladder and rectal cancer: a population based cohort study. J Urol 180 (5): 2005-9; discussion 2009-10, 2008.
- Abern MR, Dude AM, Tsivian M, et al.: The characteristics of bladder cancer after radiotherapy for prostate cancer. Urol Oncol 31 (8): 1628-34, 2013.
- Monach PA, Arnold LM, Merkel PA: Incidence and prevention of bladder toxicity from cyclophosphamide in the treatment of rheumatic diseases: a data-driven review. Arthritis Rheum 62 (1): 9-21, 2010.
- Cosyns JP: Aristolochic acid and 'Chinese herbs nephropathy': a review of the evidence to date. Drug Saf 26 (1): 33-48, 2003.
- Letašiová S, Medve'ová A, Šovčíková A, et al.: Bladder cancer, a review of the environmental risk factors. Environ Health 11 (Suppl 1): S11, 2012.
- Fernández MI, López JF, Vivaldi B, et al.: Long-term impact of arsenic in drinking water on bladder cancer health care and mortality rates 20 years after end of exposure. J Urol 187 (3): 856-61, 2012.
- Villanueva CM, Cantor KP, Grimalt JO, et al.: Bladder cancer and exposure to water disinfection by-products through ingestion, bathing, showering, and swimming in pools. Am J Epidemiol 165 (2): 148-56, 2007.
- Kantor AF, Hartge P, Hoover RN, et al.: Urinary tract infection and risk of bladder cancer. Am J Epidemiol 119 (4): 510-5, 1984.
- Locke JR, Hill DE, Walzer Y: Incidence of squamous cell carcinoma in patients with long-term catheter drainage. J Urol 133 (6): 1034-5, 1985.
- Brennan P, Bogillot O, Greiser E, et al.: The contribution of cigarette smoking to bladder cancer in women (pooled European data). Cancer Causes Control 12 (5): 411-7, 2001.
- Kirkali Z, Chan T, Manoharan M, et al.: Bladder cancer: epidemiology, staging and grading, and diagnosis. Urology 66 (6 Suppl 1): 4-34, 2005.
- Sylvester RJ, van der Meijden AP, Oosterlinck W, et al.: Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol 49 (3): 466-5; discussion 475-7, 2006.
- Herr HW: Tumor progression and survival of patients with high grade, noninvasive papillary (TaG3) bladder tumors: 15-year outcome. J Urol 163 (1): 60-1; discussion 61-2, 2000.
- Stein JP, Lieskovsky G, Cote R, et al.: Radical cystectomy in the treatment of invasive bladder cancer: long-term results in 1,054 patients. J Clin Oncol 19 (3): 666-75, 2001.
- Madersbacher S, Hochreiter W, Burkhard F, et al.: Radical cystectomy for bladder cancer today--a homogeneous series without neoadjuvant therapy. J Clin Oncol 21 (4): 690-6, 2003.
- Manoharan M, Ayyathurai R, Soloway MS: Radical cystectomy for urothelial carcinoma of the bladder: an analysis of perioperative and survival outcome. BJU Int 104 (9): 1227-32, 2009.
- Loehrer PJ, Einhorn LH, Elson PJ, et al.: A randomized comparison of cisplatin alone or in combination with methotrexate, vinblastine, and doxorubicin in patients with metastatic urothelial carcinoma: a cooperative group study. J Clin Oncol 10 (7): 1066-73, 1992.
- von der Maase H, Sengelov L, Roberts JT, et al.: Long-term survival results of a randomized trial comparing gemcitabine plus cisplatin, with methotrexate, vinblastine, doxorubicin, plus cisplatin in patients with bladder cancer. J Clin Oncol 23 (21): 4602-8, 2005.
- Millán-Rodríguez F, Chéchile-Toniolo G, Salvador-Bayarri J, et al.: Primary superficial bladder cancer risk groups according to progression, mortality and recurrence. J Urol 164 (3 Pt 1): 680-4, 2000.
- Nieder AM, Brausi M, Lamm D, et al.: Management of stage T1 tumors of the bladder: International Consensus Panel. Urology 66 (6 Suppl 1): 108-25, 2005.
- Babjuk M, Oosterlinck W, Sylvester R, et al.: EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol 54 (2): 303-14, 2008.
- Babjuk M, Oosterlinck W, Sylvester R, et al.: EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder, the 2011 update. Eur Urol 59 (6): 997-1008, 2011.
Stage Information for Bladder Cancer
The clinical staging of carcinoma of the bladder is determined by the depth of invasion of the bladder wall by the tumor. This determination requires a cystoscopic examination that includes a biopsy and examination under anesthesia to assess the following:
- Size and mobility of palpable masses.
- Degree of induration of the bladder wall.
- Presence of extravesical extension or invasion of adjacent organs.
Clinical staging, even when computed tomographic (CT) and/or magnetic resonance imaging (MRI) scans and other imaging modalities are used, often underestimates the extent of tumor, particularly in cancers that are less differentiated and more deeply invasive. CT imaging is the standard staging modality. A clinical benefit from obtaining MRI or positron emission tomography scans instead of CT imaging has not been demonstrated.[
AJCC Stage Groupings and TNM Definitions
The American Joint Committee on Cancer (AJCC) has designated staging by TNM (tumor, node, metastasis) classification to define bladder cancer.[
| Stage | TNM | Description | Illustration |
|---|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis. | |||
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | |||
| 0a | Ta, N0, M0 | Ta = Noninvasive papillary carcinoma. | 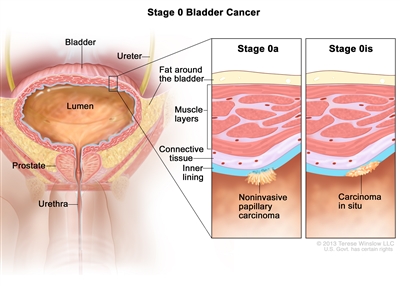 |
| N0 = No lymph node metastasis. | |||
| M0 = No distant metastasis. | |||
| 0is | Tis, N0, M0 | Tis = Urothelial carcinomain situ:flat tumor. | |
| N0 = No lymph node metastasis. | |||
| M0 = No distant metastasis. | |||
| Stage | TNM | Description | Illustration |
|---|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis. | |||
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | |||
| I | T1, N0, M0 | T1 = Tumor invades lamina propria (subepithelial connective tissue). |  |
| N0 = No lymph node metastasis | |||
| M0 = No distant metastasis. | |||
| Stage | TNM | Description | Illustration | |
|---|---|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis; p = pathological. | ||||
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | ||||
| II | T2a, N0, M0 | pT2a = Tumor invades superficial muscularis propria (inner half). |  |
|
| N0 = No lymph node metastasis. | ||||
| M0 = No distant metastasis. | ||||
| T2b, N0, M0 | pT2b = Tumor invades deep muscularis propria (outer half). | |||
| N0 = No lymph node metastasis. | ||||
| M0 = No distant metastasis. | ||||
| Stage | TNM | Description | Illustration |
|---|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis; p = pathological. | |||
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | |||
| IIIA | T3a, T3b, T4a, N0, M0 | –pT3a = Microscopically. |  |
| –pT3b = Macroscopically (extravesical mass). | |||
| –T4a = Extravesical tumor invades directly into prostatic stroma, uterus, vagina. | |||
| N0 = No lymph node metastasis. | |||
| M0 = No distant metastasis. | |||
| T1–T4a, N1, M0 | T1 = Tumor invades lamina propria (subepithelial connective tissue). | ||
| T2 = Tumor invades muscularis propria. | |||
| –pT2a = Tumor invades superficial muscularis propria (inner half). | |||
| –pT2b = Tumor invades deep muscularis propria (outer half). | |||
| T3 = Tumor invades perivesical soft tissue. | |||
| –pT3a = Microscopically. | |||
| –pT3b = Macroscopically (extravesical mass). | |||
| T4 = Extravesical tumor directly invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, pelvic wall, abdominal wall. | |||
| –T4a = Extravesical tumor invades directly into prostatic stroma, uterus, vagina. | |||
| N1 = Single regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node). | |||
| M0 = No distant metastasis. | |||
| IIIB | T1–4a, N2, N3, M0 | T1 = Tumor invades lamina propria (subepithelial connective tissue). | 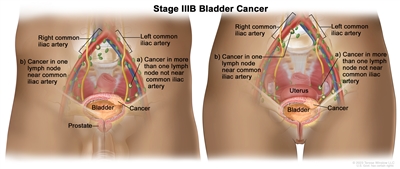 |
| T2 = Tumor invades muscularis propria. | |||
| –pT2a = Tumor invades superficial muscularis propria (inner half). | |||
| –pT2b = Tumor invades deep muscularis propria (outer half). | |||
| T3 = Tumor invades perivesical soft tissue. | |||
| –pT3a = Microscopically. | |||
| pT3b = Macroscopically (extravesical mass). | |||
| T4 = Extravesical tumor directly invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, pelvic wall, abdominal wall. | |||
| –T4a = Extravesical tumor invades directly into prostatic stroma, uterus, vagina. | |||
| N2 = Multiple regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node metastasis). | |||
| N3 = Lymph node metastasis to the common iliac lymph nodes. | |||
| M0 = No distant metastasis. | |||
| Stage | TNM | Description | Illustration |
|---|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis; p = pathological. | |||
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | |||
| IVA | T4b, N0, M0 | –T4b = Extravesical tumor invades pelvic wall, abdominal wall. | 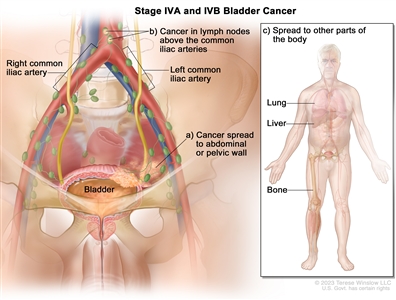 |
| N0 = No lymph node metastasis. | |||
| M0 = No distant metastasis. | |||
| Any T, Any N, M1a | TX = Primary tumor cannot be assessed. | ||
| T0 = No evidence of primary tumor. | |||
| –Ta = Noninvasive papillary carcinoma. | |||
| Tis = Urothelial carcinomain situ:flat tumor. | |||
| T1 = Tumor invades lamina propria (subepithelial connective tissue). | |||
| T2 = Tumor invades muscularis propria. | |||
| –pT2a = Tumor invades superficial muscularis propria (inner half). | |||
| –pT2b = Tumor invades deep muscularis propria (outer half). | |||
| T3 = Tumor invades perivesical soft tissue. | |||
| –pT3a = Microscopically. | |||
| –pT3b = Macroscopically (extravesical mass). | |||
| T4 = Extravesical tumor directly invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, pelvic wall, abdominal wall. | |||
| –T4a = Extravesical tumor invades directly into prostatic stroma, uterus, vagina. | |||
| –T4b = Extravesical tumor invades pelvic wall, abdominal wall. | |||
| NX = Lymph nodes cannot be assessed. | |||
| N0 = No lymph node metastasis. | |||
| N1 = Single regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node). | |||
| N2 = Multiple regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node metastasis). | |||
| N3 = Lymph node metastasis to the common iliac lymph nodes. | |||
| M0 = No distant metastasis. | |||
| –M1a = Distant metastasis limited to lymph nodes beyond the common iliacs. | |||
| IVB | Any T, Any N, M1b | TX = Primary tumor cannot be assessed. | |
| T0 = No evidence of primary tumor. | |||
| –Ta = Noninvasive papillary carcinoma. | |||
| Tis = Urothelial carcinomain situ:flat tumor. | |||
| T1 = Tumor invades lamina propria (subepithelial connective tissue). | |||
| T2 = Tumor invades muscularis propria. | |||
| –pT2a = Tumor invades superficial muscularis propria (inner half). | |||
| –pT2b = Tumor invades deep muscularis propria (outer half). | |||
| T3 = Tumor invades perivesical soft tissue. | |||
| –pT3a = Microscopically. | |||
| –pT3b = Macroscopically (extravesical mass). | |||
| T4 = Extravesical tumor directly invades any of the following: prostatic stroma, seminal vesicles, uterus, vagina, pelvic wall, abdominal wall. | |||
| –T4a = Extravesical tumor invades directly into prostatic stroma, uterus, vagina. | |||
| –T4b = Extravesical tumor invades pelvic wall, abdominal wall. | |||
| NX = Lymph nodes cannot be assessed. | |||
| N0 = No lymph node metastasis. | |||
| N1 = Single regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node). | |||
| N2 = Multiple regional lymph node metastasis in the true pelvis (perivesical, obturator, internal and external iliac, or sacral lymph node metastasis). | |||
| N3 = Lymph node metastasis to the common iliac lymph nodes. | |||
| M1b = Non-lymph node distant metastases. | |||
For urothelial histologies, a low- and high-grade designation is used to match the current World Health Organization/International Society of Urologic Pathology recommended grading system.[
For squamous cell carcinoma and adenocarcinoma, the grading schema in Table is recommended.[
| G | G Definition |
|---|---|
| a Reprinted with permission from AJCC: Urinary bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 757–65. | |
| GX | Grade cannot be assessed. |
| G1 | Well differentiated. |
| G2 | Moderately differentiated. |
| G3 | Poorly differentiated. |
References:
- Cowan NC, Crew JP: Imaging bladder cancer. Curr Opin Urol 20 (5): 409-13, 2010.
- Green DA, Durand M, Gumpeni N, et al.: Role of magnetic resonance imaging in bladder cancer: current status and emerging techniques. BJU Int 110 (10): 1463-70, 2012.
- Bochner BH, Hansel DE, Efstathiou JA, et al.: Urinary Bladder. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp 757-65.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.