Breast Cancer Treatment During Pregnancy (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Breast Cancer Treatment During Pregnancy
Incidence
Breast cancer is the most common cancer in pregnant and postpartum women and occurs in about 1 in 3,000 pregnant women. The average patient is between the ages of 32 years and 38 years. Because many women are choosing to delay childbearing, it is likely that the incidence of breast cancer during pregnancy will increase.
Anatomy
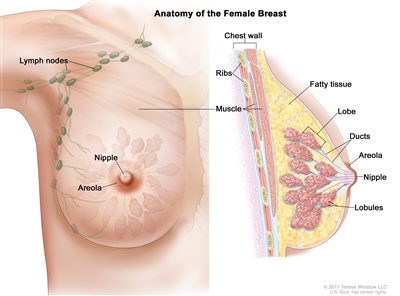
Anatomy of the female breast. The nipple and areola are shown on the outside of the breast. The lymph nodes, lobes, lobules, ducts, and other parts of the inside of the breast are also shown.
Diagnostic Evaluation
The natural tenderness and engorgement of the breasts of pregnant and lactating women may hinder detection of discrete masses and early diagnosis of breast cancer. Delays in diagnosis are common, with an average reported delay of 5 to 15 months from the onset of symptoms.[
The following tests and procedures may be used to diagnose breast cancer during pregnancy:
- Breast self-examination.
- Clinical breast examination.
- Ultrasound.
- Biopsy and hormone receptor assays.
- Mammography.
To detect breast cancer, pregnant and lactating women should consider practicing self-examination and undergo a clinical breast examination as part of the routine prenatal examination by a doctor. If an abnormality is found, diagnostic approaches such as ultrasound and mammography may be used. With proper shielding, mammography poses little risk of radiation exposure to the fetus.[
Because at least 25% of mammograms in pregnancy may be negative in the presence of cancer, a biopsy is essential for the diagnosis of any palpable mass. Diagnosis may be safely accomplished with a fine-needle aspiration, core biopsy, or excisional biopsy under local anesthesia. To avoid a false-positive diagnosis as a result of misinterpretation of pregnancy-related changes, the pathologist should be advised that the patient is pregnant.[
Breast cancer pathology is similar in age-matched pregnant and nonpregnant women. Hormone receptor assays using a competitive binding assay are usually negative in pregnant patients with breast cancer, but this may be the result of receptor binding by high serum estrogen levels associated with the pregnancy. Enzyme immunocytochemical receptor assays are more sensitive than competitive binding assays. A study that used both assay methods indicated similar receptor positivity between pregnant and nonpregnant women with breast cancer.[
For more information, see the
Prognosis
The overall survival of pregnant women with breast cancer may be worse than that of nonpregnant women at all stages.[
References:
- Hoover HC: Breast cancer during pregnancy and lactation. Surg Clin North Am 70 (5): 1151-63, 1990.
- Gwyn K, Theriault R: Breast cancer during pregnancy. Oncology (Huntingt) 15 (1): 39-46; discussion 46, 49-51, 2001.
- Moore HC, Foster RS: Breast cancer and pregnancy. Semin Oncol 27 (6): 646-53, 2000.
- Rugo HS: Management of breast cancer diagnosed during pregnancy. Curr Treat Options Oncol 4 (2): 165-73, 2003.
- Clark RM, Chua T: Breast cancer and pregnancy: the ultimate challenge. Clin Oncol (R Coll Radiol) 1 (1): 11-8, 1989.
- Yang WT, Dryden MJ, Gwyn K, et al.: Imaging of breast cancer diagnosed and treated with chemotherapy during pregnancy. Radiology 239 (1): 52-60, 2006.
- Middleton LP, Amin M, Gwyn K, et al.: Breast carcinoma in pregnant women: assessment of clinicopathologic and immunohistochemical features. Cancer 98 (5): 1055-60, 2003.
- Elledge RM, Ciocca DR, Langone G, et al.: Estrogen receptor, progesterone receptor, and HER-2/neu protein in breast cancers from pregnant patients. Cancer 71 (8): 2499-506, 1993.
- Petrek JA, Dukoff R, Rogatko A: Prognosis of pregnancy-associated breast cancer. Cancer 67 (4): 869-72, 1991.
- Barnavon Y, Wallack MK: Management of the pregnant patient with carcinoma of the breast. Surg Gynecol Obstet 171 (4): 347-52, 1990.
- Gallenberg MM, Loprinzi CL: Breast cancer and pregnancy. Semin Oncol 16 (5): 369-76, 1989.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.