Childhood Medulloblastoma and Other Central Nervous System Embryonal Tumors Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Childhood Medulloblastoma and Other Central Nervous System Embryonal Tumors
Medulloblastoma and other central nervous system (CNS) embryonal tumors may begin in embryonic (fetal) cells that remain in the brain after birth.
Medulloblastoma is a fast-growing tumor that forms in the cerebellum (the lower, back part of the brain). Medulloblastoma is the most common type of CNS embryonal tumor. CNS embryonal tumors are uncontrolled growths of cells in the brain. These tumors form in cells that are left over from fetal development, called embryonal cells. Pineoblastoma is a fast-growing type of brain tumor that forms in or around a tiny organ near the center of the brain called the pineal gland.
These tumors may be benign (not cancer) or malignant (cancer). Benign brain tumors grow and press on nearby areas of the brain but rarely spread to other parts of the brain. Malignant brain tumors are likely to grow quickly and spread into other parts of the brain. They may also spread to other parts of the body, but this is rare. When a tumor grows into and presses on an area of the brain or spreads to other parts of the brain, it may stop that part of the brain from working the way it should. Both benign and malignant brain tumors can cause serious signs or symptoms and need treatment.
Most medulloblastomas, other CNS embryonal tumors, and pineoblastomas in children are malignant. These tumors tend to spread through the cerebrospinal fluid to other parts of the brain and spinal cord.
Although cancer is rare in children, brain tumors are the second most common type of childhood cancer, after leukemia. This summary is about the treatment of primary brain tumors (tumors that begin in the brain).

Anatomy of the inside of the brain, showing the pineal and pituitary glands, optic nerve, ventricles (with cerebrospinal fluid shown in blue), and other parts of the brain.
There are different types of CNS embryonal tumors.
The different types of CNS embryonal tumors include:
| Medulloblastomas
Most CNS embryonal tumors are medulloblastomas. Medulloblastomas are fast-growing tumors that form in brain cells in the cerebellum. The cerebellum is at the lower back part of the brain between the cerebrum and the brain stem. The cerebellum controls movement, balance, and posture. It is rare for medulloblastomas to spread to the bone, bone marrow, lung, or other parts of the body. |
| Other types of CNS embryonal tumors (nonmedulloblastoma)
Other types of CNS embryonal tumors are fast-growing tumors and may form in brain cells anywhere in the brain, including the cerebrum, brain stem, or spinal cord. The cerebrum is at the top of the head and is the largest part of the brain. The cerebrum controls thinking, learning, problem-solving, emotions, speech, reading, writing, and voluntary movement. It is rare for these tumors to spread to the bone, bone marrow, lung, or other parts of the body. There are many types of CNS embryonal (nonmedulloblastoma) tumors:
|
CNS atypical teratoid/rhabdoid tumor is also a type of embryonal tumor, but it is treated differently than other childhood CNS embryonal tumors. Learn more at
Pineoblastoma forms in cells of the pineal gland.
The pineal gland is a tiny organ in the center of the brain. The gland makes melatonin, a substance that helps control our sleep cycle. Pineoblastoma are usually malignant fast-growing tumors with cells that look very different from normal pineal gland cells. Pineoblastomas are not a type of CNS embryonal tumor but treatment for them is similar to treatment for CNS embryonal tumors.
Pineoblastoma is linked with inherited changes in the retinoblastoma (RB1) gene. A child with the inherited form of retinoblastoma (cancer that forms in the tissues of the retina) has an increased risk of pineoblastoma. When retinoblastoma forms at the same time as a tumor in or near the pineal gland, it is called trilateral retinoblastoma. MRI (magnetic resonance imaging) testing in children with retinoblastoma may detect pineoblastoma at an early stage when it can be treated successfully. It is rare for pineoblastoma to spread to the bone, bone marrow, lung, or other parts of the body.
Certain genetic conditions increase the risk of childhood medulloblastoma.
Childhood medulloblastoma is caused by certain changes to the way brain cells function, especially how they grow and divide into new cells. Often, the exact cause of the cell changes is unknown. Learn more about how cancer develops at
A risk factor is anything that increases the chance of getting a disease. Not every child with one or more of these risk factors will develop medulloblastoma. And it will develop in some children who don't have a known risk factor.
The risk for medulloblastoma is increased in people who have any of the following inherited diseases:
- Turcot syndrome
- Rubinstein-Taybi syndrome
- Nevoid basal cell carcinoma (Gorlin) syndrome
- Li-Fraumeni syndrome
- Fanconi anemia
Talk with your child's doctor if you think your child may be at risk.
Genetic counseling may be done for children with medulloblastoma or pineoblastoma.
It may not be clear from the family medical history whether a child with a brain tumor has an inherited condition that increased their risk. Genetic counselors and other specially trained health professionals can discuss your child's diagnosis and the family's medical history to understand:
- your options for ELP1, APC, SUFU, PTCH1, TP53, PALB2, or BRCA2 gene testing if your child has medulloblastoma
- your options for RB1 or DICER1 gene testing if your child has pineoblastoma
- the risk of other cancers for your child
- the risk of cancer for your child's siblings
- the risks and benefits of learning genetic information
Genetic counselors can also help you cope with your child's genetic testing results, including how to discuss the results with family members.
Learn more about
Symptoms of medulloblastoma, other CNS embryonal tumors, and pineoblastoma depend on the child's age and where the tumor is.
Children may not have symptoms of medulloblastoma, other CNS embryonal tumors, or pineoblastoma until the tumor has grown bigger. It's important to check with your child's doctor if your child has:
- loss of balance, trouble walking, lack of coordination, or slow speech
- a headache, especially in the morning, or headache that goes away after vomiting
- general weakness
- weakness on one side of the face
- unusual sleepiness or change in energy level
- seizures
- double vision or other eye problems
- nausea and vomiting
Infants and young children with these tumors may be irritable or grow slowly. Also they may not eat well or meet developmental milestones such as sitting, walking, and talking in sentences. These tumors may also cause an increase in the size of an infant's head.
These symptoms may be caused by problems other than medulloblastoma, other CNS embryonal tumors, or pineoblastoma. The only way to know is to see your child's doctor.
Tests that examine the brain and spinal cord are used to diagnose childhood medulloblastoma, other CNS embryonal tumors, and pineoblastoma.
If your child has symptoms that suggest medulloblastoma, another type of CNS embryonal tumor, or pineoblastoma, the doctor will need to find out if these are due to cancer or another problem. They will ask about your child's personal and family health history and do a physical exam. Depending on the results, they may recommend other tests. If your child is diagnosed with medulloblastoma, another type of CNS embryonal tumor, or pineoblastoma, the results of these tests will help you and your child's doctor plan treatment.
The tests used to diagnose medulloblastoma, other CNS embryonal tumors, and pineoblastoma may include:
- MRI (magnetic resonance imaging) of the brain and spinal cord with gadolinium is a procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the brain and spinal cord. A substance called gadolinium is injected into a vein. The gadolinium collects around the cancer cells so they show up brighter in the picture. This procedure is also called nuclear magnetic resonance imaging (NMRI). Sometimes magnetic resonance spectroscopy (MRS) is done during the MRI scan to look at the chemicals in brain tissue.
- CT scan (CAT scan) uses a computer linked to an x-ray machine to make a series of detailed pictures inside the body from different angles. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography. Learn more about
Computed Tomography (CT) Scans and Cancer . - Lumbar puncture is a procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the lining around the spinal cord to remove a sample of CSF. The sample of CSF is checked under a microscope for signs of tumor cells. The sample may also be checked for the amounts of protein and glucose. A higher-than-normal amount of protein or lower-than-normal amount of glucose may be a sign of a tumor. This procedure is also called an LP or spinal tap.
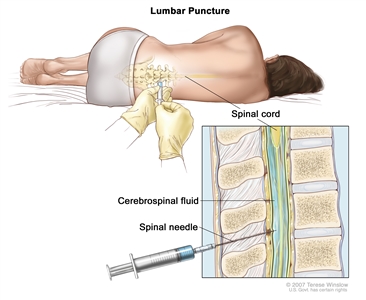
Lumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing.
A biopsy may be done to be sure of the diagnosis.
If doctors think your child may have medulloblastoma, another type of CNS embryonal tumor, or pineoblastoma, a biopsy may be done. The biopsy is done by removing part of the skull and using a needle to remove a sample of tissue. Sometimes, a computer-guided needle is used to remove the tissue sample. A pathologist views the tissue under a microscope to look for cancer cells. If cancer cells are found, the doctor may remove as much tumor as safely possible during the same surgery. The piece of skull is usually put back in place after the procedure.
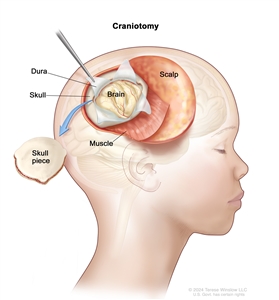
Craniotomy. An opening is made in the skull and a piece of the skull is removed to show part of the brain.
The following tests may be done on the sample of tissue that is removed:
- Immunohistochemistry is a laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient's tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
- Molecular testing checks for certain genes, proteins, or other molecules in a sample of tissue, blood, or bone marrow. Molecular tests also check for certain changes in a gene or chromosome that may cause or affect the chance of developing medulloblastoma, another type of embryonal tumor, or pineoblastoma. A molecular test may be used to help plan treatment, find out how well treatment is working, or make a prognosis. Children with medulloblastoma, another type of embryonal tumor, or pineoblastoma may be eligible for molecular testing through the Molecular Characterization Initiative.
The Molecular Characterization Initiative offers free molecular testing to children, adolescents, and young adults with certain types of newly diagnosed cancer. The program is offered through NCI's Childhood Cancer Data Initiative. To learn more, visit
About the Molecular Characterization Initiative .
Certain factors affect prognosis (chance of recovery) and treatment options.
If your child has been diagnosed with medulloblastoma, other CNS embryonal tumor, or pineoblastoma, you likely have questions about how serious the cancer is and your child's chances of survival. The likely outcome or course of a disease is called prognosis.
The prognosis and treatment options depend on:
- the type of tumor and where it is in the brain
- whether the cancer has spread within the brain and spinal cord when the tumor is found
- the age of the child when the tumor is found
- how much of the tumor remains after surgery
- whether there are certain changes in the chromosomes, genes, or brain cells
- whether the tumor has just been diagnosed or has recurred (come back)
No two people are alike, and responses to treatment can vary greatly. Your child's cancer care team is in the best position to talk with you about your child's prognosis.
You may want to get a second opinion.
You may want to get a second opinion to confirm your child's diagnosis and treatment plan. If you seek a second opinion, you will need to get important medical test results and reports from the first doctor to share with the second doctor. The second doctor will review the genetic test results, pathology report, slides, and scans. This doctor may agree with the first doctor, suggest changes to the treatment plan, or provide more information about your child's tumor.
To learn more about choosing a doctor and getting a second opinion, see
Staging Childhood Medulloblastoma, Other Central Nervous System Embryonal Tumors, and Pineoblastoma
Medulloblastoma, other CNS embryonal tumors, and pineoblastoma in children are treated based on the tumor type and the child's age.
Cancer stage describes the extent of cancer in the body, such as the size of the tumor, whether it has spread, and how far it has spread from where it first formed. There is no staging system used for childhood medulloblastoma, other central nervous system (CNS) embryonal tumors, or pineoblastoma, but the tests and procedures done to diagnose the cancer are also used to help plan treatment.
Treatment of other CNS embryonal tumors and pineoblastoma in children is based on the child's age. Children aged 3 years and younger may be given different treatment than children older than 3 years.
Treatment of medulloblastoma in children older than 3 years also depends on whether the tumor is average risk or high risk.
Average risk
Medulloblastomas are called average risk when all of the following are true:
- The tumor was completely removed by surgery or there was only a very small amount remaining.
- The cancer has not spread to other parts of the body.
High risk
Medulloblastomas are called high risk if any of the following are true:
- Some of the tumor was not removed by surgery.
- The cancer has spread to other parts of the brain or spinal cord or to other parts of the body.
In general, cancer is more likely to recur (come back) after treatment in patients with a high-risk tumor.
The results of the tests and procedures done to diagnose medulloblastoma, other CNS embryonal tumors, and pineoblastoma in children are used to plan cancer treatment.
If your child is diagnosed with medulloblastoma, another type of CNS embryonal tumor, or pineoblastoma, they will be referred to a pediatric oncologist /neuro-oncologist. This is a doctor who specializes in staging and treating childhood cancers. They will recommend tests to determine the extent (stage) of cancer. Some of the tests used to diagnose the cancer are repeated after surgery. This is to find out how much tumor remains after surgery and to see if the cancer has spread from the brain to the spine or other parts of the body. It is important to know if the cancer has spread in order to plan the best treatment. Learn more about diagnostic tests in the
The following tests may be used to find out if the cancer has spread beyond the brain and spinal cord:
- Bone marrow aspiration and biopsy are procedures in which a sample of bone marrow and bone is removed from the hipbone or breastbone using a special needle. A pathologist views the sample under a microscope to look for signs of cancer. A bone marrow aspiration and biopsy are only done when there are signs the cancer has spread to the bone marrow.
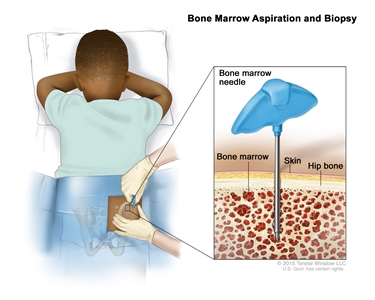
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child's hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope. - Bone scan is a procedure to check if there are rapidly dividing cells, such as cancer cells, in the bone. A very small amount of radioactive material is injected into a vein and travels through the bloodstream. The radioactive material collects in the bones with cancer and is detected by a scanner. A bone scan is only done when there are signs or symptoms that the cancer has spread to the bone.
Sometimes childhood medulloblastoma and other central nervous system embryonal tumors come back after treatment.
Childhood medulloblastoma and other types of CNS embryonal tumors most often recur (come back) within 3 years after treatment but may come back many years later. Recurrent childhood medulloblastoma and other CNS embryonal tumors may come back in the same place as the original tumor and/or in a different place in the brain or spinal cord.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.