Endometrial Cancer Treatment (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Endometrial Cancer
Cancer of the endometrium is the most common gynecologic malignancy in the United States and accounts for 7% of all cancers in women. Most cases are diagnosed at an early stage and are amenable to treatment with surgery alone.[
Incidence and Mortality
Estimated new cases and deaths from cancer of the uterine corpus, which includes the endometrium, in the United States in 2025:[
- New cases: 69,120.
- Deaths: 13,860.
Anatomy
The endometrium is the inner lining of the uterus and has both functional and basal layers. The functional layer is hormonally sensitive and is shed in a cyclical pattern during menstruation in reproductive-age women. Both estrogen and progesterone are necessary to maintain a normal endometrial lining. However, factors that lead to an excess of estrogen, including obesity and anovulation, lead to an increase in the deposition of the endometrial lining. These changes may lead to endometrial hyperplasia and, in some cases, endometrial cancer. Whatever the cause, a thickened lining will lead to sloughing of the endometrial tissue through the endometrial canal and into the vagina. As a result, heavy menstrual bleeding or bleeding after menopause are often the initial signs of endometrial cancer. This symptom tends to happen early in the disease course, allowing for identification of the disease at an early stage for most women.
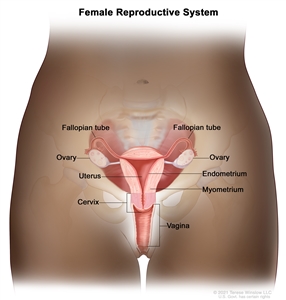
Anatomy of the female reproductive system.
Risk Factors
Increasing age is the most important risk factor for most cancers. Other risk factors for endometrial cancer include the following:
- Hormone therapy.[
3 ,4 ,5 ,6 ]- Postmenopausal estrogen therapy.[
7 ,8 ,9 ,10 ,11 ,12 ,13 ,14 ]
- Postmenopausal estrogen therapy.[
- Selective estrogen receptor modifiers.[
15 ,16 ,17 ]- Tamoxifen therapy.
- Obesity.[
18 ,19 ] - Metabolic syndrome.[
20 ] - Diabetes.[
21 ,22 ] - Reproductive factors.
- Nulliparity.[
23 ] - Early menarche or late menopause.[
24 ] - Polycystic ovary syndrome.[
25 ]
- Nulliparity.[
- Family history/genetic predisposition.
- Mother, sister, or daughter with uterine cancer.[
26 ] - Certain genetic syndromes, such as Lynch syndrome.[
27 ,28 ,29 ,30 ]
- Mother, sister, or daughter with uterine cancer.[
- Endometrial hyperplasia.[
31 ]
For more information, see
Prolonged, unopposed estrogen exposure has been associated with an increased risk of endometrial cancer.[
Tamoxifen, which is used to treat and prevent breast cancer (
Clinical Features
Irregular vaginal bleeding is the most common presenting sign of endometrial cancer. It generally occurs early in the disease process and is the reason why most patients are diagnosed with highly curable stage I endometrial cancer.
Diagnostic Evaluation
The following procedures may be used to detect endometrial cancer:
- Transvaginal ultrasonography.
- Endometrial biopsy.
- Pelvic examination.
- Dilatation and curettage.
- Hysteroscopy.
To definitively diagnose endometrial cancer, a procedure that directly samples the endometrial tissue is necessary.
The Pap smear is not a reliable screening procedure for the detection of endometrial cancer, even though a retrospective study found a strong correlation between positive cervical cytology and high-risk endometrial disease (i.e., high-grade tumor and deep myometrial invasion).[
Prognostic Factors
Prognostic factors for endometrial cancer include:
-
Tumor stage and grade (including extrauterine nodal spread) . -
Hormone receptor status .
Tumor stage and grade (including extrauterine nodal spread)
| Prognostic Group | Patient Characteristics | Risk of Nodal Involvement |
|---|---|---|
| A | Grade 1 tumors involving only endometrium | <5% |
| No evidence of intraperitoneal spread | ||
| B | Grade 2–3 tumors | 5%–9% pelvic nodes |
| Invasion of <50% of myometrium | ||
| No intraperitoneal spread | 4% para-aortic nodes | |
| C | Deep muscle invasion | 20%–60% pelvic nodes |
| High-grade tumors | 10%–30% para-aortic nodes | |
| Intraperitoneal spread |
A Gynecologic Oncology Group study related surgical-pathological parameters and postoperative treatment to recurrence-free interval and recurrence site. Grade 3 histology and deep myometrial invasion in patients without extrauterine spread were the greatest determinants of recurrence. In this study, the presence of the following factors greatly increased the frequency of recurrence:[
- Positive pelvic nodes.
- Adnexal metastasis.
- Positive peritoneal cytology.
- Capillary space involvement.
- Involvement of the isthmus or cervix.
- Positive para-aortic nodes (includes all grades and depth of invasion). Of the cases with aortic node metastases, 98% were in patients with positive pelvic nodes, intra-abdominal metastases, or tumor invasion of the outer 33% of the myometrium.
When the only evidence of extrauterine spread is positive peritoneal cytology, the influence on outcome is unclear. The value of therapy directed at this cytological finding is not well founded,[
Involvement of the capillary-lymphatic space on histopathological examination correlates with extrauterine and nodal spread of tumor.[
Hormone receptor status
When possible, progesterone and estrogen receptor statuses, assessed either by biochemical or immunohistochemical methods, are included in the evaluation of patients with stage I and stage II cancer.[
One report found progesterone receptor levels to be the single most important prognostic indicator of 3-year survival in clinical stages I and II disease. Patients with progesterone receptor levels of 100 or greater had a 3-year disease-free survival rate of 93%, compared with 36% for those with a level below 100. After adjusting for progesterone receptor levels, only cervical involvement and peritoneal cytology were significant prognostic variables.[
Other reports confirm the importance of hormone receptor status as an independent prognostic factor.[
Other prognostic factors
Other factors predictive of poor prognosis include:[
- A high S-phase fraction.
- Aneuploidy.
- PTEN loss-of-function variant.
- PIK3CA variant.
- TP53 variant.
- Oncogene expression (e.g., overexpression of the HER2/neu oncogene has been associated with a poor overall prognosis).
A general review of prognostic factors has been published.[
References:
- American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025.
Available online . Last accessed January 16, 2025. - Ward KK, Shah NR, Saenz CC, et al.: Cardiovascular disease is the leading cause of death among endometrial cancer patients. Gynecol Oncol 126 (2): 176-9, 2012.
- Beral V, Bull D, Reeves G, et al.: Endometrial cancer and hormone-replacement therapy in the Million Women Study. Lancet 365 (9470): 1543-51, 2005 Apr 30-May 6.
- Anderson GL, Limacher M, Assaf AR, et al.: Effects of conjugated equine estrogen in postmenopausal women with hysterectomy: the Women's Health Initiative randomized controlled trial. JAMA 291 (14): 1701-12, 2004.
- Furness S, Roberts H, Marjoribanks J, et al.: Hormone therapy in postmenopausal women and risk of endometrial hyperplasia. Cochrane Database Syst Rev (2): CD000402, 2009.
- Grady D, Gebretsadik T, Kerlikowske K, et al.: Hormone replacement therapy and endometrial cancer risk: a meta-analysis. Obstet Gynecol 85 (2): 304-13, 1995.
- Smith DC, Prentice R, Thompson DJ, et al.: Association of exogenous estrogen and endometrial carcinoma. N Engl J Med 293 (23): 1164-7, 1975.
- Mack TM, Pike MC, Henderson BE, et al.: Estrogens and endometrial cancer in a retirement community. N Engl J Med 294 (23): 1262-7, 1976.
- Ziel HK, Finkle WD: Increased risk of endometrial carcinoma among users of conjugated estrogens. N Engl J Med 293 (23): 1167-70, 1975.
- Walker AM, Jick H: Cancer of the corpus uteri: increasing incidence in the United States, 1970--1975. Am J Epidemiol 110 (1): 47-51, 1979.
- Gray LA, Christopherson WM, Hoover RN: Estrogens and endometrial carcinoma. Obstet Gynecol 49 (4): 385-9, 1977.
- McDonald TW, Annegers JF, O'Fallon WM, et al.: Exogenous estrogen and endometrial carcinoma: case-control and incidence study. Am J Obstet Gynecol 127 (6): 572-80, 1977.
- Antunes CM, Strolley PD, Rosenshein NB, et al.: Endometrial cancer and estrogen use. Report of a large case-control study. N Engl J Med 300 (1): 9-13, 1979.
- Shapiro S, Kelly JP, Rosenberg L, et al.: Risk of localized and widespread endometrial cancer in relation to recent and discontinued use of conjugated estrogens. N Engl J Med 313 (16): 969-72, 1985.
- Fisher B, Costantino JP, Redmond CK, et al.: Endometrial cancer in tamoxifen-treated breast cancer patients: findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-14. J Natl Cancer Inst 86 (7): 527-37, 1994.
- Cummings SR, Eckert S, Krueger KA, et al.: The effect of raloxifene on risk of breast cancer in postmenopausal women: results from the MORE randomized trial. Multiple Outcomes of Raloxifene Evaluation. JAMA 281 (23): 2189-97, 1999.
- DeMichele A, Troxel AB, Berlin JA, et al.: Impact of raloxifene or tamoxifen use on endometrial cancer risk: a population-based case-control study. J Clin Oncol 26 (25): 4151-9, 2008.
- Bergström A, Pisani P, Tenet V, et al.: Overweight as an avoidable cause of cancer in Europe. Int J Cancer 91 (3): 421-30, 2001.
- Aune D, Navarro Rosenblatt DA, Chan DS, et al.: Anthropometric factors and endometrial cancer risk: a systematic review and dose-response meta-analysis of prospective studies. Ann Oncol 26 (8): 1635-48, 2015.
- Esposito K, Chiodini P, Capuano A, et al.: Metabolic syndrome and endometrial cancer: a meta-analysis. Endocrine 45 (1): 28-36, 2014.
- Troisi R, Potischman N, Hoover RN, et al.: Insulin and endometrial cancer. Am J Epidemiol 146 (6): 476-82, 1997.
- Tsilidis KK, Kasimis JC, Lopez DS, et al.: Type 2 diabetes and cancer: umbrella review of meta-analyses of observational studies. BMJ 350: g7607, 2015.
- Dossus L, Allen N, Kaaks R, et al.: Reproductive risk factors and endometrial cancer: the European Prospective Investigation into Cancer and Nutrition. Int J Cancer 127 (2): 442-51, 2010.
- Brown SB, Hankinson SE: Endogenous estrogens and the risk of breast, endometrial, and ovarian cancers. Steroids 99 (Pt A): 8-10, 2015.
- Barry JA, Azizia MM, Hardiman PJ: Risk of endometrial, ovarian and breast cancer in women with polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod Update 20 (5): 748-58, 2014 Sep-Oct.
- Win AK, Reece JC, Ryan S: Family history and risk of endometrial cancer: a systematic review and meta-analysis. Obstet Gynecol 125 (1): 89-98, 2015.
- Daniels MS: Genetic testing by cancer site: uterus. Cancer J 18 (4): 338-42, 2012 Jul-Aug.
- Dunlop MG, Farrington SM, Nicholl I, et al.: Population carrier frequency of hMSH2 and hMLH1 mutations. Br J Cancer 83 (12): 1643-5, 2000.
- Lynch HT, Lynch J, Conway T, et al.: Familial aggregation of carcinoma of the endometrium. Am J Obstet Gynecol 171 (1): 24-7, 1994.
- Lu KH, Schorge JO, Rodabaugh KJ, et al.: Prospective determination of prevalence of lynch syndrome in young women with endometrial cancer. J Clin Oncol 25 (33): 5158-64, 2007.
- Widra EA, Dunton CJ, McHugh M, et al.: Endometrial hyperplasia and the risk of carcinoma. Int J Gynecol Cancer 5 (3): 233-235, 1995.
- Jick SS, Walker AM, Jick H: Estrogens, progesterone, and endometrial cancer. Epidemiology 4 (1): 20-4, 1993.
- Jick SS: Combined estrogen and progesterone use and endometrial cancer. Epidemiology 4 (4): 384, 1993.
- Bilezikian JP: Major issues regarding estrogen replacement therapy in postmenopausal women. J Womens Health 3 (4): 273-82, 1994.
- van Leeuwen FE, Benraadt J, Coebergh JW, et al.: Risk of endometrial cancer after tamoxifen treatment of breast cancer. Lancet 343 (8895): 448-52, 1994.
- DuBeshter B, Warshal DP, Angel C, et al.: Endometrial carcinoma: the relevance of cervical cytology. Obstet Gynecol 77 (3): 458-62, 1991.
- Larson DM, Johnson KK, Reyes CN, et al.: Prognostic significance of malignant cervical cytology in patients with endometrial cancer. Obstet Gynecol 84 (3): 399-403, 1994.
- Takeshima N, Hirai Y, Tanaka N, et al.: Pelvic lymph node metastasis in endometrial cancer with no myometrial invasion. Obstet Gynecol 88 (2): 280-2, 1996.
- Morrow CP, Bundy BN, Kurman RJ, et al.: Relationship between surgical-pathological risk factors and outcome in clinical stage I and II carcinoma of the endometrium: a Gynecologic Oncology Group study. Gynecol Oncol 40 (1): 55-65, 1991.
- Lanciano RM, Corn BW, Schultz DJ, et al.: The justification for a surgical staging system in endometrial carcinoma. Radiother Oncol 28 (3): 189-96, 1993.
- Ambros RA, Kurman RJ: Combined assessment of vascular and myometrial invasion as a model to predict prognosis in stage I endometrioid adenocarcinoma of the uterine corpus. Cancer 69 (6): 1424-31, 1992.
- Turner DA, Gershenson DM, Atkinson N, et al.: The prognostic significance of peritoneal cytology for stage I endometrial cancer. Obstet Gynecol 74 (5): 775-80, 1989.
- Piver MS, Recio FO, Baker TR, et al.: A prospective trial of progesterone therapy for malignant peritoneal cytology in patients with endometrial carcinoma. Gynecol Oncol 47 (3): 373-6, 1992.
- Kadar N, Homesley HD, Malfetano JH: Positive peritoneal cytology is an adverse factor in endometrial carcinoma only if there is other evidence of extrauterine disease. Gynecol Oncol 46 (2): 145-9, 1992.
- Lurain JR: The significance of positive peritoneal cytology in endometrial cancer. Gynecol Oncol 46 (2): 143-4, 1992.
- Lurain JR, Rice BL, Rademaker AW, et al.: Prognostic factors associated with recurrence in clinical stage I adenocarcinoma of the endometrium. Obstet Gynecol 78 (1): 63-9, 1991.
- Garg G, Gao F, Wright JD, et al.: Positive peritoneal cytology is an independent risk-factor in early stage endometrial cancer. Gynecol Oncol 128 (1): 77-82, 2013.
- Hanson MB, van Nagell JR, Powell DE, et al.: The prognostic significance of lymph-vascular space invasion in stage I endometrial cancer. Cancer 55 (8): 1753-7, 1985.
- Carcangiu ML, Chambers JT, Voynick IM, et al.: Immunohistochemical evaluation of estrogen and progesterone receptor content in 183 patients with endometrial carcinoma. Part I: Clinical and histologic correlations. Am J Clin Pathol 94 (3): 247-54, 1990.
- Chambers JT, Carcangiu ML, Voynick IM, et al.: Immunohistochemical evaluation of estrogen and progesterone receptor content in 183 patients with endometrial carcinoma. Part II: Correlation between biochemical and immunohistochemical methods and survival. Am J Clin Pathol 94 (3): 255-60, 1990.
- Gurpide E: Endometrial cancer: biochemical and clinical correlates. J Natl Cancer Inst 83 (6): 405-16, 1991.
- Ingram SS, Rosenman J, Heath R, et al.: The predictive value of progesterone receptor levels in endometrial cancer. Int J Radiat Oncol Biol Phys 17 (1): 21-7, 1989.
- Creasman WT: Prognostic significance of hormone receptors in endometrial cancer. Cancer 71 (4 Suppl): 1467-70, 1993.
- Friberg LG, Norén H, Delle U: Prognostic value of DNA ploidy and S-phase fraction in endometrial cancer stage I and II: a prospective 5-year survival study. Gynecol Oncol 53 (1): 64-9, 1994.
- Hetzel DJ, Wilson TO, Keeney GL, et al.: HER-2/neu expression: a major prognostic factor in endometrial cancer. Gynecol Oncol 47 (2): 179-85, 1992.
- Binder PS, Mutch DG: Update on prognostic markers for endometrial cancer. Womens Health (Lond Engl) 10 (3): 277-88, 2014.
Stage Information for Endometrial Cancer
The pattern of endometrial cancer spread is partially dependent on the degree of cellular differentiation. Well-differentiated tumors tend to limit their spread to the surface of the endometrium; myometrial invasion is less common. Myometrial invasion occurs much more frequently in patients with poorly differentiated tumors and is frequently a harbinger of lymph node involvement and distant metastases.[
Metastatic spread occurs in a characteristic pattern. Regional spread to the pelvic and para-aortic nodes is common. Distant metastasis most commonly involves the following sites:
- Lungs.
- Inguinal and supraclavicular nodes.
- Liver.
- Bones.
- Brain.
- Vagina.
FIGO Staging
The Fédération Internationale de Gynécologie et d'Obstétrique (FIGO) and the American Joint Committee on Cancer (AJCC) have both designated staging systems for endometrial cancer. The FIGO system is the most commonly used staging system for endometrial cancer.[
FIGO stages I to IV are further subdivided by the histological grade (G) of the tumor, for example, stage IB G2. Carcinosarcomas, which had previously been designated as sarcomas, are now considered poorly differentiated adenocarcinomas; as such, they are included in this system.[
2023 FIGO staging for endometrial cancer
| Stage | Description | |
|---|---|---|
| T = primary tumor; N = regional lymph node; M = distant metastasis; p = pathological; AJCC = American Joint Committee on Cancer; ESGO-ESTRO-ESP = European Society of Gynaecological Oncology, European Society for Radiotherapy and Oncology, European Society of Pathology; FIGO = Fédération Internationale de Gynécologie et d'Obstétrique; ITC = isolated tumor cell; LVSI = lymphovascular space involvement; MMRd = mismatch repair deficiency; NSMP = no specific molecular profile;POLEmut= pathogenicPOLEmutation; p53abn =TP53abnormal; SLN = sentinel lymph node; WHO = World Health Organization. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| b Endometrial cancer is surgically staged and pathologically examined. In all stages, the grade of the lesion, the histological type and LVSI must be recorded. If available and feasible, molecular classification testing (POLEmut, MMRd, NSMP, p53abn) is encouraged in all patients with endometrial cancer for prognostic risk-group stratification and as factors that might influence adjuvant and systemic treatment decisions (see |
||
| c In early endometrial cancer, the standard surgery is a total hysterectomy with bilateral salpingo-oophorectomy via a minimally invasive laparoscopic approach. Staging procedures include infracolic omentectomy in specific histological subtypes, such as serous and undifferentiated endometrial carcinoma, as well as carcinosarcoma, due to the high risk of microscopic omental metastases. Lymph node staging should be performed in patients with intermediate-high/high-risk disease. SLN biopsy is an adequate alternative to systematic lymphadenectomy for staging proposes. SLN biopsy can also be considered in patients with low−/low-intermediate-risk disease to rule out occult lymph node metastases and to identify disease truly confined to the uterus. Thus, the ESGO-ESTRO-ESP guidelines allow an approach of SLN in all patients with endometrial carcinoma, which is endorsed by FIGO. In assumed early endometrial cancer, an SLN biopsy in an adequate alternative to systematic lymphadenectomy in high-intermediate and high-risk cases for the purpose of lymph node staging and can also be considered in low–/intermediate-risk disease to rule out occult lymph node metastases. An SLN biopsy should be done in association with thorough (ultrastaging) staging as it will increase the detection of low-volume disease in lymph nodes. | ||
| d Low-grade endometrioid carcinomas involving both the endometrium and the ovary are considered to have a good prognosis, and no adjuvant treatment is recommended if all the below criteria are met. Disease limited to low-grade endometrioid carcinomas involving the endometrium and ovaries (Stage IA3) must be distinguished from extensive spread of the endometrial carcinoma to the ovary (Stage IIIA1), by the following criteria: (1) no more than superficial myometrial invasion is present (<50%); (2) absence of extensive/substantial LVSI; (3) absence of additional metastases; and (4) the ovarian tumor is unilateral, limited to the ovary, without capsule invasion/rupture (equivalent to pT1a). | ||
| e LVSI as defined in WHO 2021: extensive/substantial, ≥5 vessels involved. | ||
| f Grade and histological type are as follows: (1) Serous adenocarcinomas, clear cell adenocarcinomas, mesonephric-like carcinomas, gastrointestinal-type mucinous endometrial carcinoma, undifferentiated carcinomas, and carcinosarcomas are considered high grade by definition. For endometrioid carcinomas, grade is based on the proportion of solid areas: low grade = grade 1 (≤5%) and grade 2 (6%–50%); and high grade = grade 3 (>50%). Nuclear atypia excessive for the grade raises the grade of a grade 1 or 2 tumor by one. The presence of unusual nuclear atypia in an architecturally low-grade tumor should prompt the evaluation ofTP53and consideration of serous carcinoma. Adenocarcinomas with squamous differentiation are graded according to the microscopic features of the glandular component; (2) Nonaggressive histological types are composed of low-grade (grade 1 and 2) endometrioid carcinomas. Aggressive histological types are composed of high-grade endometrioid carcinomas (grade 3), serous, clear cell, undifferentiated, mixed, mesonephric-like, gastrointestinal mucinous type carcinomas, and carcinosarcomas; and (3) It should be noted that high-grade endometrioid carcinomas (grade 3) are a prognostically, clinically, and molecularly heterogenous disease, and the tumor type that benefits most from applying molecular classification for improved prognostication and for treatment decision-making. Without molecular classification, high-grade endometrioid carcinomas cannot appropriately be allocated to a risk group, and thus, molecular profiling is particularly recommended in these patients. For practical purposes and to avoid undertreatment of patients, if the molecular classification is unknown, high-grade endometrioid carcinomas were grouped together with the aggressive histological types in the actual FIGO classification. | ||
| g Micrometastases are considered to be metastatic involvement (pN1 [mi]). The prognostic significance of ITCs is unclear. The presence of ITCs should be documented and is regarded as pN0(I+). According to the AJCC 8th edition staging, macrometastases are >2 mm in size, micrometastases are >0.2–2 mm and/or >200 cells, and ITCs are ≤0.2 mm and ≤200 cells. These definitions are based on staging established by FIGO and the 8th edition of the AJCC Cancer Staging Manual. | ||
| I | Confined to the uterine corpus and ovary.d | |
| IA | Disease limited to the endometrium OR nonaggressive histological type, i.e., low-grade endometrioid, with invasion of less than half of myometrium with no or focal LVSI OR good prognosis disease. | |
| IA1 | Nonaggressive histological type limited to an endometrial polyp OR confined to the endometrium. | |
| IA2 | Nonaggressive histological types involving less than half of the myometrium with no or focal LVSI. | |
| IA3 | Low-grade endometrioid carcinomas limited to the uterus and ovary.d | |
| IB | Nonaggressive histological types with invasion of half or more of the myometrium, and with no or focal LVSI.e | |
| IC | Aggressive histological typesf limited to a polyp or confined to the endometrium. | |
| Stage | Description |
|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique; LVSI = lymphovascular space involvement. | |
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
|
| For the explanations for footnotesb−f, see |
|
| II | Invasion of cervical stroma without extrauterine extension OR with substantial LVSI OR aggressive histological types with myometrial invasion. |
| IIA | Invasion of the cervical stroma of nonaggressive histological types. |
| IIB | Substantial LVSIe of nonaggressive histological types. |
| IIC | Aggressive histological typesf with any myometrial involvement. |
| Stage | Description | |
|---|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| For the explanations for footnotesb−d andg, see |
||
| III | Local and/or regional spread of the tumor of any histological subtype. | |
| IIIA | Invasion of uterine serosa, adnexa, or both by direct extension or metastasis. | |
| IIIA1 | Spread to ovary or fallopian tube (except when meeting stage IA3 criteria).d | |
| IIIA2 | Involvement of uterine subserosa or spread through the uterine serosa. | |
| IIIB | Metastasis or direct spread to the vagina and/or to the parametria or pelvic peritoneum. | |
| IIIB1 | Metastasis or direct spread to the vagina and/or the parametria. | |
| IIIB2 | Metastasis to the pelvic peritoneum. | |
| IIIC | Metastasis to the pelvic or para-aortic lymph nodes or both.g | |
| IIIC1 | Metastasis to the pelvic lymph nodes. | |
| IIIC1i | Micrometastasis. | |
| IIIC1ii | Macrometastasis. | |
| IIIC2 | Metastasis to para-aortic lymph nodes up to the renal vessels, with or without metastasis to the pelvic lymph nodes. | |
| IIIC2i | Micrometastasis. | |
| IIIC2ii | Macrometastasis. | |
| Stage | Description |
|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | |
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
|
| For the explanations for footnotesb−c, see |
|
| IV | Spread to the bladder mucosa and/or intestinal mucosa and/or distance metastasis. |
| IVA | Invasion of the bladder mucosa and/or the intestinal/bowel mucosa. |
| IVB | Abdominal peritoneal metastasis beyond the pelvis. |
| IVC | Distant metastasis, including metastasis to any extra- or intra-abdominal lymph nodes above the renal vessels, lungs, liver, brain, or bone. |
| Stage Designation | Molecular Findings in Patients With Early Endometrial Cancer (Stages I and II After Surgical Staging) |
|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique; LVSI = lymphovascular space involvement; MMRd = mismatch repair deficiency; MSI = microsatellite instability; NSMP = no specific molecular profile;POLEmut= pathogenicPOLEmutation; p53abn =TP53abnormal. | |
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
|
| b When feasible, the addition of molecular subtype to the staging criteria allows a better prediction of prognosis in a staging/prognosis scheme. The performance of complete molecular classification (POLEmut, MMRd, NSMP, p53abn) is encouraged in all cases of endometrial cancer for prognostic risk-group stratification and as potential influencing factors of adjuvant or systemic treatment decisions. Molecular subtype assignment can be done on a biopsy, in which case it need not be repeated on the hysterectomy specimen. When performed, these molecular classifications should be recorded in all stages. A pathogenicPOLEmutation (POLEmut) is associated with a good prognosis. MMRd or MSI and NSMP are associated with an intermediate prognosis. AbnormalTP53(p53abn) is associated with a poor prognosis. When the molecular classification is known the staging is modified as follows: (1) FIGO Stages I and II are based on surgical/anatomical and histological findings. In case the molecular classification revealsPOLEmutor p53abn status, the FIGO stage is modified in the early stage of the disease. This is depicted in the FIGO stage by the addition of "m" for molecular classification, and a subscript is added to denotePOLEmutor p53abn status, as shown in the table. MMRd or NSMP status do not modify early FIGO stages; however, these molecular classifications should be recorded for the purpose of data collection. When molecular classification reveals MMRd or NSMP, it should be recorded as Stage ImMMRd or Stage ImNSMP and Stage IImMMRd or Stage IImNSMP; (2) FIGO Stages III and IV are based on surgical/anatomical findings. The stage category is not modified by molecular classification; however, the molecular classification should be recorded if known. When the molecular classification is known, it should be recorded as Stage IIIm or Stage IVm with the appropriate subscript for the purpose of data collection. For example, when molecular classification reveals p53abn, it should be recorded as Stage IIImp53abn or Stage IVmp53abn. | |
| IAmPOLEmut | POLEmutendometrial carcinoma, confined to the uterine corpus or with cervical extension, regardless of the degree of LVSI or histological type. |
| IICmp53abn | p53abn endometrial carcinoma confined to the uterine corpus with any myometrial invasion, with or without cervical invasion, and regardless of the degree of LVSI or histological type. |
2021 FIGO staging for endometrial cancer
| Stage | Description | Illustration |
|---|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| b G1, G2, or G3 (G = grade). | ||
| Ib | Tumor confined to the corpus uteri. | 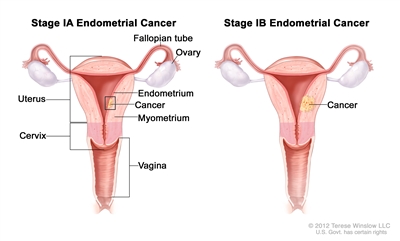 |
| IAb | No or less than half myometrial invasion. | |
| IBb | Invasion equal to or more than half of the myometrium. | |
| Stage | Description | Illustration |
|---|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| b G1, G2, or G3 (G = grade). | ||
| c Endocervical glandular involvement is considered stage I; it is no longer considered stage II. | ||
| IIb | Tumor invades cervical stroma but does not extend beyond the uterus.c | 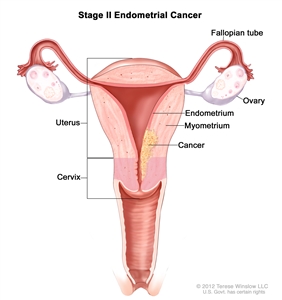 |
| Stage | Description | Illustration |
|---|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| b G1, G2, or G3 (G = grade). | ||
| c Positive cytology has to be reported separately without changing the stage. | ||
| IIIb | Local and/or regional spread of the tumor. | |
| IIIAb | Tumor invades the serosa of the corpus uteri and/or adnexae.c | 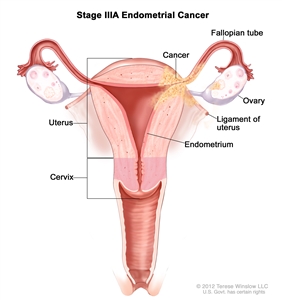 |
| IIIBb | Vaginal and/or parametrial involvement.c | 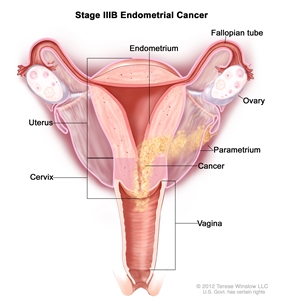 |
| IIICb | Metastases to pelvic and/or para-aortic lymph nodes.c | 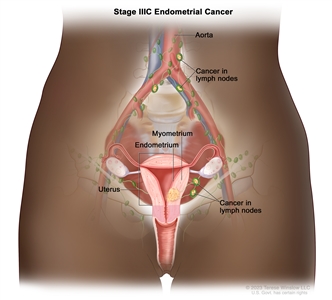 |
| IIIC1b | Positive pelvic nodes. | |
| IIIC2b | Positive para-aortic lymph nodes with or without positive pelvic lymph nodes. | |
| Stage | Description | Illustration |
|---|---|---|
| FIGO = Fédération Internationale de Gynécologie et d'Obstétrique. | ||
| a Adapted from FIGO Committee on Gynecologic Oncology.[ |
||
| b G1, G2, or G3 (G = grade). | ||
| IVb | Tumor invades bladder and/or bowel mucosa, and/or distant metastases. | |
| IVAb | Tumor invasion of bladder and/or bowel mucosa. | 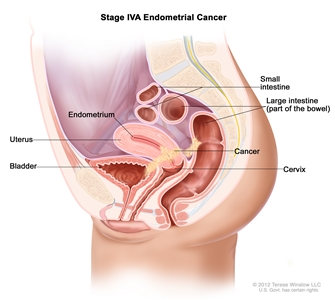 |
| IVBb | Distant metastases, including intra-abdominal metastases and/or inguinal lymph nodes. | 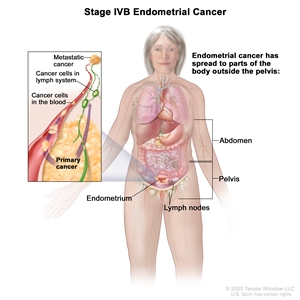 |
References:
- Hendrickson M, Ross J, Eifel PJ, et al.: Adenocarcinoma of the endometrium: analysis of 256 cases with carcinoma limited to the uterine corpus. Pathology review and analysis of prognostic variables. Gynecol Oncol 13 (3): 373-92, 1982.
- Nori D, Hilaris BS, Tome M, et al.: Combined surgery and radiation in endometrial carcinoma: an analysis of prognostic factors. Int J Radiat Oncol Biol Phys 13 (4): 489-97, 1987.
- Berek JS, Matias-Guiu X, Creutzberg C, et al.: FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet 162 (2): 383-394, 2023.
- Koskas M, Amant F, Mirza MR, et al.: Cancer of the corpus uteri: 2021 update. Int J Gynaecol Obstet 155 (Suppl 1): 45-60, 2021.
- Corpus uteri – carcinoma and carcinosarcoma. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp 661-69.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.