Genetics of Gastric Cancer (PDQ®): Genetics - Health Professional Information [NCI]
Introduction
Gastric cancer is one of the most commonly diagnosed cancers in the world, with an incidence of over 1 million cases and an estimated 769,000 deaths occurring in 2020. Globally, this cancer ranked fifth for cancer incidence and fourth for cancer mortality in 2020.[
The genes that can predispose individuals to hereditary diffuse gastric cancer (HDGC) include the following:
-
CDH1 . -
CTNNA1 .
HDGC is the most common hereditary cancer syndrome that can predispose individuals to gastric cancer. This disease does not have an easily detectable precursor lesion. For more information, see
There are also hereditary cancer syndromes that can cause other forms of gastric cancer. These syndromes include the following:
- Lynch syndrome: Lynch syndrome is caused by pathogenic variants in MLH1, MSH2, MSH6, PMS2, and EPCAM. The amount of gastric cancer risk associated with Lynch syndrome and the role of gastric cancer screening remain unknown, especially since a Lynch syndrome–associated gastric cancer precursor has not yet been identified.[
6 ] - Familial adenomatous polyposis (FAP)/gastric adenocarcinoma and proximal polyposis of the stomach (GAPPS): FAP/GAPPS are caused by pathogenic variants in APC. Gastric cancer is typically preceded by fundic gland polyps.[
7 ] - Peutz-Jeghers syndrome (PJS): PJS is caused by pathogenic variants in STK11. Gastric cancer is typically preceded by hamartomatous polyps.[
8 ] - Juvenile polyposis syndrome (JPS): JPS is caused by pathogenic variants in SMAD4 and BMPR1A. Gastric cancer is typically preceded by hamartomatous polyps.
In each of these syndromes, gastric polyps and gastric cancer risk are of secondary importance to colorectal polyps and colorectal cancer. Gastric polyp burden (including polyp count and size) and gastric cancer risk may vary between individuals.
For more information on these genetic syndromes, see
Gastric Cancer Risk Factors
Environmental risk factors
Incidence rates for gastric cancer are the highest in Eastern Asia and Eastern Europe, while the rates in Northern America, Northern Europe, and Africa are generally low.[
Environmental risk factors for gastric cancer include the following:
1. Helicobacter pylori (H. pylori) infection.
- This may be most the impactful environmental risk factor for gastric cancer.
- An H. pylori infection may cause histological changes in the stomach, which can begin with chronic, active gastritis and can progress to gastric atrophy, intestinal metaplasia, gastric dysplasia, and eventually gastric cancer.[
9 ,10 ] - The combination of H. pylori and germline pathogenic variants in homologous recombination genes (ATM, BRCA1, BRCA2, and PALB2) increases the risk of gastric cancer in an additive manner. A study of 38,153 controls and 10,426 gastric cancer cases in Japan found that germline pathogenic variants in nine genes (APC, ATM, BRCA1, BRCA2, CDH1, MLH1, MSH2, MSH6, and PALB2) were associated with increased gastric cancer risk.[
11 ] The relative risk (RR) of gastric cancer in those with H. pylori and a pathogenic variant in one of four homologous recombination genes was 16.01 (confidence interval, 2.22–29.8). Risk persisted after adjusting for environmental risk factors like smoking, obesity, and salt intake. There was no increased risk in those who had H. pylori and a pathogenic variant in a mismatch repair gene. The authors noted that results primarily pertain to the Japanese population, since gastric cancer and H. pylori incidence rates are much higher in East Asian populations than in Western populations.
2. Diet.
- The regional variation in gastric cancer incidence is influenced by diet.[
12 ,13 ] - Gastric cancer risk may increase when individuals consume foods that are preserved with salt.[
13 ,14 ] - Low fruit intake and the consumption of a large amount of processed, grilled, or barbequed meats/fish may also increase gastric cancer risk.[
13 ]
3. Migrant effects.
- Gastric cancer risk may also be affected by migrant effects (i.e., effects incurred when individuals migrate from a region with high gastric cancer risk to a region with low gastric cancer risk or vice versa).
- Studies have demonstrated that the incidence of gastric cancer in immigrants correlates closely with the incidence of gastric cancer in their new host country after one or two generations.[
15 ,16 ,17 ]
4. Tobacco use.[
5. Alcohol use.[
6. Emerging evidence for obesity and gastroesophageal reflux disease (GERD).
- Emerging evidence suggests an association between increased gastric cancer risk, excess body weight, and tissue damage associated with GERD.[
18 ,19 ]
7. Racial and ethnic disparities.
- There are striking racial and ethnic disparities associated with gastric cancer incidence in the United States.[
20 ,21 ,22 ,23 ,24 ,25 ] - Studies that examine genetic and nongenetic risk factors, such as social determinants of health, are needed to understand and reduce the disparities in gastric cancer incidence that are seen in different racial and ethnic minority groups.
Intensive surveillance may be clinically warranted in individuals with hereditary, environmental, or ethnicity-based gastric cancer risk factors. However, more data are needed to show whether these risk factors increase or decrease gastric cancer risk in individuals with hereditary gastric cancer pathogenic variants. For more information about risk factors for gastric cancer in the general population, see
Familial risk factors
Individuals with family histories of gastric cancer have an increased risk of developing gastric cancer.[
Families with multiple gastric cancer cases have also been used to study the heritability of gastric cancer. A report in 1964 described a large, native Maori family from New Zealand.[
Precancerous Lesions
In the stomach, gastric adenocarcinoma can arise from visible lesions, from the histological progression of mucosal atrophy or, less commonly, from invisible lesions (i.e., submucosal infiltration, as seen in diffuse-type gastric adenocarcinoma). This section reviews both gastric polyps and the histological changes associated with chronic gastritis that can predispose an individual to gastric cancer.
Gastric polyps
Gastric polyps are common in the U.S. population and are found in up to 6% of individuals who undergo endoscopy. However, these polyps rarely progress to become gastric cancer.[
- Adenomatous.
- Hyperplastic.
- Inflammatory.
- Hamartomatous (associated with PJS, JPS, and PTEN hamartoma tumor syndromes [PHTS]).
- Fundic gland.[
42 ]
In general, the malignant potential of a polyp is determined by the polyp's histology, size, and degree of dysplasia, if present. Adenomatous and hyperplastic polyps have the highest malignant potentials, especially when H. pylori is present. In contrast, fundic gland polyps (with or without dysplasia) rarely progress to become gastric cancer, even in individuals who have FAP.[
Fundic gland polyps of the stomach are common and typically associated with long-term proton pump inhibitor (PPI) use.[
Inflammatory and hyperplastic polyps can present with many different pathological features. Unlike the colon, in which hyperplastic polyps carry little or no cancer risk, hyperplastic polyps of the stomach can enlarge and develop dysplastic foci.[
Hamartomatous polyps are seen in the stomachs of patients with PJS, JPS, and PHTS. For more information on these hereditary cancer syndromes, see
Gastric adenomas make up approximately 10% of all gastric polyps. A gastric adenoma's malignant potential is determined by its histological subtype and size.[
Chronic gastritis
Chronic gastritis, a histological diagnosis defined by the presence of a mononuclear cellular infiltrate in the lamina propria of the stomach, occurs due to environmental exposures or autoimmune gastritis. Chronic gastritis can lead to gastric intestinal metaplasia. H. pylori is the most common risk factor for intestinal metaplasia. Other risk factors for intestinal metaplasia include pernicious anemia, autoimmune gastritis, ethnicity, a family history of gastric cancer, dietary habits, smoking, and alcohol use.[
The steps of Correa's cascade include the following:
- Chronic gastritis (most commonly caused by H. pylori).
- Gastric mucosal atrophy.
- Gastric intestinal metaplasia.
- Gastric dysplasia (low-grade dysplasia followed by high-grade dysplasia).[
50 ,51 ]
Although these histological changes are associated with increased gastric cancer risk in the general population, the prevalence of findings and associated cancer risk in hereditary cancer syndromes is unknown. Each step in Correa's cascade only occurs in a minority of patients. There is considerable controversy regarding appropriate surveillance in patients with intestinal metaplasia.[
Endoscopic assessment
Gastric cancer screening is not routinely performed in the United States, where gastric cancer incidence is relatively low. Gastric cancer screening is also not usually performed in individuals with family histories of gastric cancer in which a hereditary gastric cancer pathogenic variant has not been identified. Large, prospective multicenter studies are needed to determine if gastric cancer screening programs would improve mortality in individuals from the United States with family histories of gastric cancer. In the United States, gastric cancer surveillance guidelines only exist for individuals with pathogenic variants in CDH1 or other gastric cancer risk genes (for more information, see
When evaluating any patient with hereditary gastric cancer risk, endoscopy includes assessment for gastric polyps and H. pylori —despite a lack of evidence demonstrating that H. pylori increases gastric cancer risk in the setting of all hereditary cancer syndromes.[
A small focus of intestinal metaplasia in the antrum is shown below. Intestinal metaplasia is not always visible on endoscopy. Instead, it is often found when taking random biopsies of the stomach.[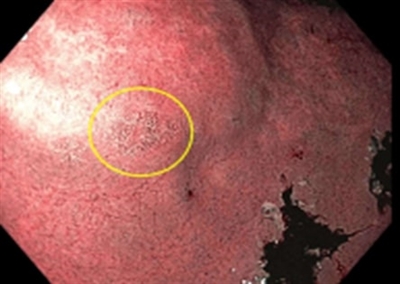
Endoscopic image showing a small area of intestinal metaplasia (circled in yellow) in the antrum of the stomach.
References:
- Allemani C, Matsuda T, Di Carlo V, et al.: Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 391 (10125): 1023-1075, 2018.
- Sung H, Ferlay J, Siegel RL, et al.: Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin 71 (3): 209-249, 2021.
- American Cancer Society: Cancer Facts and Figures 2024. American Cancer Society, 2024.
Available online . Last accessed December 30, 2024. - Uson PLS, Kunze KL, Golafshar MA, et al.: Germline Cancer Testing in Unselected Patients with Gastric and Esophageal Cancers: A Multi-center Prospective Study. Dig Dis Sci 67 (11): 5107-5115, 2022.
- Ku GY, Kemel Y, Maron SB, et al.: Prevalence of Germline Alterations on Targeted Tumor-Normal Sequencing of Esophagogastric Cancer. JAMA Netw Open 4 (7): e2114753, 2021.
- Møller P, Seppälä TT, Bernstein I, et al.: Cancer risk and survival in path_MMR carriers by gene and gender up to 75 years of age: a report from the Prospective Lynch Syndrome Database. Gut 67 (7): 1306-1316, 2018.
- Abraham SC, Nobukawa B, Giardiello FM, et al.: Fundic gland polyps in familial adenomatous polyposis: neoplasms with frequent somatic adenomatous polyposis coli gene alterations. Am J Pathol 157 (3): 747-54, 2000.
- Giardiello FM, Brensinger JD, Tersmette AC, et al.: Very high risk of cancer in familial Peutz-Jeghers syndrome. Gastroenterology 119 (6): 1447-53, 2000.
- Correa P, Haenszel W, Cuello C, et al.: A model for gastric cancer epidemiology. Lancet 2 (7924): 58-60, 1975.
- Hooi JKY, Lai WY, Ng WK, et al.: Global Prevalence of Helicobacter pylori Infection: Systematic Review and Meta-Analysis. Gastroenterology 153 (2): 420-429, 2017.
- Usui Y, Taniyama Y, Endo M, et al.: Helicobacter pylori, Homologous-Recombination Genes, and Gastric Cancer. N Engl J Med 388 (13): 1181-1190, 2023.
- Tsugane S, Sasazuki S: Diet and the risk of gastric cancer: review of epidemiological evidence. Gastric Cancer 10 (2): 75-83, 2007.
- Liu SJ, Huang PD, Xu JM, et al.: Diet and gastric cancer risk: an umbrella review of systematic reviews and meta-analyses of prospective cohort studies. J Cancer Res Clin Oncol 148 (8): 1855-1868, 2022.
- Song Y, Liu X, Cheng W, et al.: The global, regional and national burden of stomach cancer and its attributable risk factors from 1990 to 2019. Sci Rep 12 (1): 11542, 2022.
- Shimizu H, Mack TM, Ross RK, et al.: Cancer of the gastrointestinal tract among Japanese and white immigrants in Los Angeles County. J Natl Cancer Inst 78 (2): 223-8, 1987.
- Mousavi SM, Brandt A, Weires M, et al.: Cancer incidence among Iranian immigrants in Sweden and Iranian residents compared to the native Swedish population. Eur J Cancer 46 (3): 599-605, 2010.
- Lee J, Demissie K, Lu SE, et al.: Cancer incidence among Korean-American immigrants in the United States and native Koreans in South Korea. Cancer Control 14 (1): 78-85, 2007.
- Bouras E, Tsilidis KK, Triggi M, et al.: Diet and Risk of Gastric Cancer: An Umbrella Review. Nutrients 14 (9): , 2022.
- Poly TN, Lin MC, Syed-Abdul S, et al.: Proton Pump Inhibitor Use and Risk of Gastric Cancer: Current Evidence from Epidemiological Studies and Critical Appraisal. Cancers (Basel) 14 (13): , 2022.
- Shah SC, McKinley M, Gupta S, et al.: Population-Based Analysis of Differences in Gastric Cancer Incidence Among Races and Ethnicities in Individuals Age 50 Years and Older. Gastroenterology 159 (5): 1705-1714.e2, 2020.
- Anderson WF, Rabkin CS, Turner N, et al.: The Changing Face of Noncardia Gastric Cancer Incidence Among US Non-Hispanic Whites. J Natl Cancer Inst 110 (6): 608-615, 2018.
- Islami F, DeSantis CE, Jemal A: Incidence Trends of Esophageal and Gastric Cancer Subtypes by Race, Ethnicity, and Age in the United States, 1997-2014. Clin Gastroenterol Hepatol 17 (3): 429-439, 2019.
- Holowatyj AN, Ulrich CM, Lewis MA: Racial/Ethnic Patterns of Young-Onset Noncardia Gastric Cancer. Cancer Prev Res (Phila) 12 (11): 771-780, 2019.
- De B, Rhome R, Jairam V, et al.: Gastric adenocarcinoma in young adult patients: patterns of care and survival in the United States. Gastric Cancer 21 (6): 889-899, 2018.
- Gupta S, Tao L, Murphy JD, et al.: Race/Ethnicity-, Socioeconomic Status-, and Anatomic Subsite-Specific Risks for Gastric Cancer. Gastroenterology 156 (1): 59-62.e4, 2019.
- Hemminki K, Sundquist J, Ji J: Familial risk for gastric carcinoma: an updated study from Sweden. Br J Cancer 96 (8): 1272-7, 2007.
- Yaghoobi M, Bijarchi R, Narod SA: Family history and the risk of gastric cancer. Br J Cancer 102 (2): 237-42, 2010.
- Lissowska J, Groves FD, Sobin LH, et al.: Family history and risk of stomach cancer in Warsaw, Poland. Eur J Cancer Prev 8 (3): 223-7, 1999.
- Palli D, Russo A, Ottini L, et al.: Red meat, family history, and increased risk of gastric cancer with microsatellite instability. Cancer Res 61 (14): 5415-9, 2001.
- Dhillon PK, Farrow DC, Vaughan TL, et al.: Family history of cancer and risk of esophageal and gastric cancers in the United States. Int J Cancer 93 (1): 148-52, 2001.
- Minami Y, Tateno H: Associations between cigarette smoking and the risk of four leading cancers in Miyagi Prefecture, Japan: a multi-site case-control study. Cancer Sci 94 (6): 540-7, 2003.
- Eto K, Ohyama S, Yamaguchi T, et al.: Familial clustering in subgroups of gastric cancer stratified by histology, age group and location. Eur J Surg Oncol 32 (7): 743-8, 2006.
- Chen MJ, Wu DC, Ko YC, et al.: Personal history and family history as a predictor of gastric cardiac adenocarcinoma risk: a case-control study in Taiwan. Am J Gastroenterol 99 (7): 1250-7, 2004.
- Yatsuya H, Toyoshima H, Tamakoshi A, et al.: Individual and joint impact of family history and Helicobacter pylori infection on the risk of stomach cancer: a nested case-control study. Br J Cancer 91 (5): 929-34, 2004.
- Lichtenstein P, Holm NV, Verkasalo PK, et al.: Environmental and heritable factors in the causation of cancer--analyses of cohorts of twins from Sweden, Denmark, and Finland. N Engl J Med 343 (2): 78-85, 2000.
- JONES EG: FAMILIAL GASTRIC CANCER. N Z Med J 63: 287-96, 1964.
- Guilford P, Hopkins J, Harraway J, et al.: E-cadherin germline mutations in familial gastric cancer. Nature 392 (6674): 402-5, 1998.
- Guilford PJ, Hopkins JB, Grady WM, et al.: E-cadherin germline mutations define an inherited cancer syndrome dominated by diffuse gastric cancer. Hum Mutat 14 (3): 249-55, 1999.
- Corso G, Marrelli D, Pascale V, et al.: Frequency of CDH1 germline mutations in gastric carcinoma coming from high- and low-risk areas: metanalysis and systematic review of the literature. BMC Cancer 12: 8, 2012.
- Brooks-Wilson AR, Kaurah P, Suriano G, et al.: Germline E-cadherin mutations in hereditary diffuse gastric cancer: assessment of 42 new families and review of genetic screening criteria. J Med Genet 41 (7): 508-17, 2004.
- Carmack SW, Genta RM, Schuler CM, et al.: The current spectrum of gastric polyps: a 1-year national study of over 120,000 patients. Am J Gastroenterol 104 (6): 1524-32, 2009.
- Gullo I, Grillo F, Mastracci L, et al.: Precancerous lesions of the stomach, gastric cancer and hereditary gastric cancer syndromes. Pathologica 112 (3): 166-185, 2020.
- Mankaney G, Leone P, Cruise M, et al.: Gastric cancer in FAP: a concerning rise in incidence. Fam Cancer 16 (3): 371-376, 2017.
- Martin FC, Chenevix-Trench G, Yeomans ND: Systematic review with meta-analysis: fundic gland polyps and proton pump inhibitors. Aliment Pharmacol Ther 44 (9): 915-925, 2016.
- Jain R, Chetty R: Gastric hyperplastic polyps: a review. Dig Dis Sci 54 (9): 1839-46, 2009.
- Stolte M, Sticht T, Eidt S, et al.: Frequency, location, and age and sex distribution of various types of gastric polyp. Endoscopy 26 (8): 659-65, 1994.
- Abraham SC, Park SJ, Lee JH, et al.: Genetic alterations in gastric adenomas of intestinal and foveolar phenotypes. Mod Pathol 16 (8): 786-95, 2003.
- Chen ZM, Scudiere JR, Abraham SC, et al.: Pyloric gland adenoma: an entity distinct from gastric foveolar type adenoma. Am J Surg Pathol 33 (2): 186-93, 2009.
- Altayar O, Davitkov P, Shah SC, et al.: AGA Technical Review on Gastric Intestinal Metaplasia-Epidemiology and Risk Factors. Gastroenterology 158 (3): 732-744.e16, 2020.
- Correa P: Human gastric carcinogenesis: a multistep and multifactorial process--First American Cancer Society Award Lecture on Cancer Epidemiology and Prevention. Cancer Res 52 (24): 6735-40, 1992.
- Neumann WL, Coss E, Rugge M, et al.: Autoimmune atrophic gastritis--pathogenesis, pathology and management. Nat Rev Gastroenterol Hepatol 10 (9): 529-41, 2013.
- Dinis-Ribeiro M, Kuipers EJ: How to Manage a Patient With Gastric Intestinal Metaplasia: An International Perspective. Gastroenterology 158 (6): 1534-1537, 2020.
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Colorectal. Version 1.2023. Plymouth Meeting, PA: National Comprehensive Cancer Network, 2023.
Available with free registration. Last accessed June 28, 2023. - National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 3.2023. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2023.
Available online with free registration. Last accessed October 17, 2024. - Blair VR, McLeod M, Carneiro F, et al.: Hereditary diffuse gastric cancer: updated clinical practice guidelines. Lancet Oncol 21 (8): e386-e397, 2020.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.