Hereditary Diffuse Gastric Cancer (PDQ®): Genetics - Health Professional Information [NCI]
Clinical Manifestations
Gastric Cancer Risk
In CDH1pathogenic variant carriers, lifetime risk of diffuse gastric cancer by age 80 years ranges from 37% to 70% in men and 25% to 83% in women.[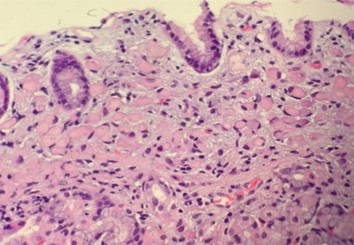
Figure 1. High-power image of a gastric biopsy tissue sample showing signet ring cell carcinoma. Note the absence of gland formation, which indicates that this lesion is poorly-differentiated carcinoma. Also note the overlying epithelium, which although effaced by the presence of underlying tumor, is otherwise normal.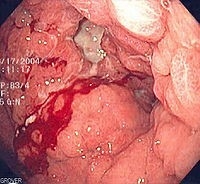
Figure 2. Endoscopic image of diffuse gastric cancer with typical linitis plastica involvement. This occurs at an advanced stage. The gastric mucosa and submucosa are diffusely infiltrated such that the entire stomach becomes stiff, losing contractility and the ability to digest food. This leads to the typical symptoms of nausea and vomiting. Biopsy is generally informative, but a very superficial biopsy may be negative for cancer cells. Hence, it is imperative for pathologists to carefully search biopsy specimens for isolated signet ring cells.
Breast Cancer Risk
In the general population, most breast cancers are ductal, while about 10% are lobular.[
References:
- Pharoah PD, Guilford P, Caldas C, et al.: Incidence of gastric cancer and breast cancer in CDH1 (E-cadherin) mutation carriers from hereditary diffuse gastric cancer families. Gastroenterology 121 (6): 1348-53, 2001.
- Roberts ME, Ranola JMO, Marshall ML, et al.: Comparison of CDH1 Penetrance Estimates in Clinically Ascertained Families vs Families Ascertained for Multiple Gastric Cancers. JAMA Oncol 5 (9): 1325-1331, 2019.
- Xicola RM, Li S, Rodriguez N, et al.: Clinical features and cancer risk in families with pathogenic CDH1 variants irrespective of clinical criteria. J Med Genet 56 (12): 838-843, 2019.
- Hansford S, Kaurah P, Li-Chang H, et al.: Hereditary Diffuse Gastric Cancer Syndrome: CDH1 Mutations and Beyond. JAMA Oncol 1 (1): 23-32, 2015.
- Delgado E, León-Ponte M, Villahermosa ML, et al.: Analysis of HIV type 1 protease and reverse transcriptase sequences from Venezuela for drug resistance-associated mutations and subtype classification: a UNAIDS study. AIDS Res Hum Retroviruses 17 (8): 753-8, 2001.
- Caldas C, Carneiro F, Lynch HT, et al.: Familial gastric cancer: overview and guidelines for management. J Med Genet 36 (12): 873-80, 1999.
- Li CI, Anderson BO, Daling JR, et al.: Trends in incidence rates of invasive lobular and ductal breast carcinoma. JAMA 289 (11): 1421-4, 2003.
- Corso G, Intra M, Trentin C, et al.: CDH1 germline mutations and hereditary lobular breast cancer. Fam Cancer 15 (2): 215-9, 2016.
- Corso G, Figueiredo J, La Vecchia C, et al.: Hereditary lobular breast cancer with an emphasis on E-cadherin genetic defect. J Med Genet 55 (7): 431-441, 2018.
- Masciari S, Larsson N, Senz J, et al.: Germline E-cadherin mutations in familial lobular breast cancer. J Med Genet 44 (11): 726-31, 2007.
- Kaurah P, MacMillan A, Boyd N, et al.: Founder and recurrent CDH1 mutations in families with hereditary diffuse gastric cancer. JAMA 297 (21): 2360-72, 2007.
- Mouabbi JA, Hassan A, Lim B, et al.: Invasive lobular carcinoma: an understudied emergent subtype of breast cancer. Breast Cancer Res Treat 193 (2): 253-264, 2022.
- Pilonis ND, Tischkowitz M, Fitzgerald RC, et al.: Hereditary Diffuse Gastric Cancer: Approaches to Screening, Surveillance, and Treatment. Annu Rev Med 72: 263-280, 2021.
- Rakha EA, El-Sayed ME, Powe DG, et al.: Invasive lobular carcinoma of the breast: response to hormonal therapy and outcomes. Eur J Cancer 44 (1): 73-83, 2008.
- Lamovec J, Bracko M: Metastatic pattern of infiltrating lobular carcinoma of the breast: an autopsy study. J Surg Oncol 48 (1): 28-33, 1991.
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Breast Cancer. Version 4.2023. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2023.
Available online with free registration. Last accessed October 25, 2024.
Management
Surgical Intervention: Risk-Reducing Gastrectomy
Risk-reducing total gastrectomy (RRTG) with esophagojejunostomy remains the treatment of choice for individuals with CDH1pathogenic variants.[
Functional outcomes after RRTG vary, but weight loss is universal. One series reported an average weight loss of 15% to 20% postsurgery.[
An international group of experts have published consensus guidelines for follow-up of patients with hereditary diffuse gastric cancer (HDGC) after RRTG.[
Endoscopic Surveillance
RRTG is generally considered the treatment of choice for patients with HDGC since it minimizes gastric cancer risk by removing high-risk gastric tissue (given the lack of consistently identifiable precursor lesions on endoscopy).[
Although RRTG remains the gold standard recommendation for HDGC, a multidisciplinary discussion on management options is favored based on the following: emerging evidence on endoscopic surveillance, the unpredictable rate of progression from intramucosal signet cells and T1a lesions to advanced gastric cancer, and morbidity of surgery. There is a role for endoscopic surveillance in HDGC, specifically for patients who decline surgery or choose to defer RRTG when they are diagnosed with HDGC. A prospective cohort study analyzed 270 asymptomatic CDH1 carriers (median age, 46.6 y; interquartile range [IQR], 36.5–59.8) who declined RRTG and participated in endoscopic surveillance with the Cambridge protocol (9%) or Bethesda protocol (91%).[
Other scenarios that may prompt endoscopic surveillance include the following:[
- Patients with family histories suggestive of HDGC but for whom no pathogenic variant has been identified.
- Patients with family histories of intestinal-type gastric cancer. This type of gastric cancer is usually not associated with CDH1 pathogenic variants. Therefore, endoscopic surveillance needs to be individualized for these patients.
- Patients who have a CDH1 pathogenic variant and choose to defer RRTG for a year or more. This includes patients who undergo genetic testing at a young age and test positive for a CDH1 pathogenic variant. Risk-reducing gastrectomy is generally not recommended in individuals who are younger than 18 to 20 years. Despite being warned about endoscopic biopsy's poor rate of HDGC precursor detection, many patients (especially those who are older) will only consider gastrectomy in the event of a positive biopsy.
There are no definitive, identifiable features of early diffuse gastric cancer or diffuse gastric cancer precursors that can be found on endoscopy. Targeted biopsies of ulcers, erythema, nodularity/nodules, polyps, erosions, and scars revealed SSRC in less than 10% of samples.[
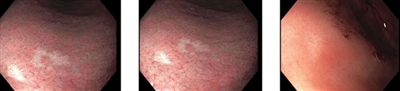
Figure 3. Several small, white, slightly depressed areas are best seen with narrow-band imaging. These lesions can resemble scars from previous endoscopic biopsies. However, the images above are from a patient who did not have a prior esophagogastroduodenoscopy. A microscopic signet ring cell carcinoma focus was found on this biopsy, although nontargeted biopsies in this patient were also positive for signet ring cell carcinoma.
Another study reported on 33 patients with CDH1 pathogenic variants (median age, 32 y) who were members of the original Māori family in which HDGC was first discovered. Participants underwent 99 surveillance endoscopies, 93 of which were performed with a mucolytic N-acetylcysteine followed by Congo red–methylene blue dye.[
If an endoscopic approach is taken for HDGC management, endoscopic surveillance is recommended annually unless signet ring cell features are found. If signet ring cell lesions are found on endoscopy, discussion with a multidisciplinary team is warranted.[
Breast Cancer Risk Management
In females with a CDH1 pathogenic variant, screening modalities for breast cancer include the following:
Breast magnetic resonance imaging (MRI):
- The National Comprehensive Cancer Network (NCCN) recommends consideration of breast MRI with contrast beginning at age 30 years.[
17 ] - The International Gastric Cancer Linkage Consortium (IGCLC) recommends that annual breast MRI begin at age 30 years since mammography is not effective at identifying lobular breast cancer.[
1 ,18 ]
Mammography:
- NCCN and IGCLC have differing recommendations regarding the age to begin mammography screening.
- NCCN recommends that annual mammography screenings begin at age 30 years.[
17 ] - IGCLC recommends that annual mammography screenings begin between the ages of 35 and 40 years, based on the patient's breast cancer risk factors, like breast density.[
1 ]
Other imaging:
- The IGCLC states that supplementary screening of dense breasts with ultrasound can be considered, especially when MRI is not available, contraindicated, or declined.[
1 ]
Bilateral risk-reducing mastectomy can be considered for women with a CDH1 pathogenic variant based on a strong family history of breast cancer, additional breast cancer risk factors, and/or personal choice.[
References:
- Blair VR, McLeod M, Carneiro F, et al.: Hereditary diffuse gastric cancer: updated clinical practice guidelines. Lancet Oncol 21 (8): e386-e397, 2020.
- Vos EL, Salo-Mullen EE, Tang LH, et al.: Indications for Total Gastrectomy in CDH1 Mutation Carriers and Outcomes of Risk-Reducing Minimally Invasive and Open Gastrectomies. JAMA Surg 155 (11): 1050-1057, 2020.
- Strong VE, Gholami S, Shah MA, et al.: Total Gastrectomy for Hereditary Diffuse Gastric Cancer at a Single Center: Postsurgical Outcomes in 41 Patients. Ann Surg 266 (6): 1006-1012, 2017.
- Stillman MD, Kusche N, Toledano S, et al.: Short and long-term outcomes of prophylactic total gastrectomy in 54 consecutive individuals with germline pathogenic mutations in the CDH1 gene. J Surg Oncol 126 (8): 1413-1422, 2022.
- Asif B, Sarvestani AL, Gamble LA, et al.: Cancer surveillance as an alternative to prophylactic total gastrectomy in hereditary diffuse gastric cancer: a prospective cohort study. Lancet Oncol 24 (4): 383-391, 2023.
- Charlton A, Blair V, Shaw D, et al.: Hereditary diffuse gastric cancer: predominance of multiple foci of signet ring cell carcinoma in distal stomach and transitional zone. Gut 53 (6): 814-20, 2004.
- van der Post RS, Gullo I, Oliveira C, et al.: Histopathological, Molecular, and Genetic Profile of Hereditary Diffuse Gastric Cancer: Current Knowledge and Challenges for the Future. Adv Exp Med Biol 908: 371-91, 2016.
- Corso G, Magnoni F, Nicastro V, et al.: Global distribution of prophylactic total gastrectomy in E-cadherin (CDH1) mutations. Semin Oncol 49 (2): 130-135, 2022.
- Bres C, Voron T, Benhaim L, et al.: Management of Pathogenic CDH1 Variant Carriers Within the FREGAT Network: A Multicentric Retrospective Study. Ann Surg 276 (5): 830-837, 2022.
- Davis JL, Ripley RT: Postgastrectomy Syndromes and Nutritional Considerations Following Gastric Surgery. Surg Clin North Am 97 (2): 277-293, 2017.
- Roberts G, Benusiglio PR, Bisseling T, et al.: International Delphi consensus guidelines for follow-up after prophylactic total gastrectomy: the Life after Prophylactic Total Gastrectomy (LAP-TG) study. Gastric Cancer 25 (6): 1094-1104, 2022.
- Norton JA, Ham CM, Van Dam J, et al.: CDH1 truncating mutations in the E-cadherin gene: an indication for total gastrectomy to treat hereditary diffuse gastric cancer. Ann Surg 245 (6): 873-9, 2007.
- Jacobs MF, Dust H, Koeppe E, et al.: Outcomes of Endoscopic Surveillance in Individuals With Genetic Predisposition to Hereditary Diffuse Gastric Cancer. Gastroenterology 157 (1): 87-96, 2019.
- Lee CYC, Olivier A, Honing J, et al.: Endoscopic surveillance with systematic random biopsy for the early diagnosis of hereditary diffuse gastric cancer: a prospective 16-year longitudinal cohort study. Lancet Oncol 24 (1): 107-116, 2023.
- Fujita H, Lennerz JK, Chung DC, et al.: Endoscopic surveillance of patients with hereditary diffuse gastric cancer: biopsy recommendations after topographic distribution of cancer foci in a series of 10 CDH1-mutated gastrectomies. Am J Surg Pathol 36 (11): 1709-17, 2012.
- Shaw D, Blair V, Framp A, et al.: Chromoendoscopic surveillance in hereditary diffuse gastric cancer: an alternative to prophylactic gastrectomy? Gut 54 (4): 461-8, 2005.
- National Comprehensive Cancer Network: NCCN Clinical Practice Guidelines in Oncology: Genetic/Familial High-Risk Assessment: Breast, Ovarian, and Pancreatic. Version 2.2024. Plymouth Meeting, Pa: National Comprehensive Cancer Network, 2023.
Available online with free registration. Last accessed September 18, 2024. - Pereslucha AM, Wenger DM, Morris MF, et al.: Invasive Lobular Carcinoma: A Review of Imaging Modalities with Special Focus on Pathology Concordance. Healthcare (Basel) 11 (5): , 2023.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.