Informal Caregivers in Cancer: Roles, Burden, and Support (PDQ®): Supportive care - Health Professional Information [NCI]
Caregiver Burden
The term caregiver burden describes a caregiver's perceptions of the demands of caregiving and the resources available for addressing those demands. The Transactional Model of Stress and Coping is a useful framework for describing the relationships among caregiver demands, resources, burden, and the psychological consequences of being burdened.[
The process begins with the primary appraisal, which is a judgment about the relevance of the health threat and any demands on the caregiver. A demand that is judged to be relevant receives a secondary appraisal to evaluate the likelihood that available resources have the potential to reduce or overcome the demand. Burden is perceived to be high when the difficulty of the demand outweighs the available resources. Coping strategies may also determine whether the psychological consequences of the perceived burden are negative or positive.
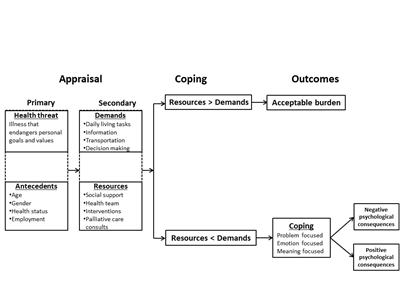
The Transactional Model of Stress and Coping may explain why some caregivers experience burden and negative psychological consequences. Clinicians may intervene to reduce demands, increase resources, or foster adoptive coping. The text for antecedents, demands, and resources is from examples in the text of this summary.
The Transactional Model of Stress and Coping shown above has not been validated and serves to organize the remainder of the summary.
Primary Appraisal: Demands on Informal Caregivers
Qualitative analysis of interviews: A mixed-methods study of 48 informal caregivers of patients undergoing chemotherapy demonstrated several notable findings.[
One group of investigators interviewed six patients with head and neck cancer and their spouses within 6 months of completing treatment. Thematic analysis demonstrated several unmet needs, including the following:[
- Better preparation for side effects.
- Clearer timeline of recovery.
- Strategies to deal with the emotions experienced by patients and spouses during treatment.
The complexity of a caregiver's life is further highlighted in a systematic review of qualitative studies of informal caregivers of patients with cancer and symptoms or signs of cachexia.[
- Impact on everyday life.
- Attempts of caregiver to take charge.
- Need for health care provider input.
- Conflict with patient.
- Negative emotions.
Surveys: To provide a more-accurate assessment of the needs of caregivers, one group of investigators developed and demonstrated the psychometric validity of the Supportive Care Needs Survey—Partners and Caregivers (SCNS–P&C).[
The diagnoses of survivors included the following:
- Prostate cancer (32%).
- Blood cancers (16.3%).
- Breast cancer (13.2%).
- Melanoma (11.5%).
- Colorectal cancer (11.3%).
- Head and neck cancer (8.6%).
- Lung cancer (7.1%).
Analysis revealed four domains of needs:
- Health care service.
- Psychological and emotional.
- Work and social.
- Information.
Investigators using the SCNS–P&C to conduct a telephone survey of 196 caregivers of patients with renal cell carcinoma demonstrated that 64% of caregivers had at least one significant unmet need; 53% had three or more unmet needs; and 29% had ten or more unmet needs.[
- Health care service, 30%.
- Psychological and emotional, 30%.
- Work and social, 23%.
- Informational, 18%.
In another study, 188 patient-caregiver dyads completed the SCNS–P&C.[
- Support in managing fears about the patient's condition.
- Receiving disease-related information.
- Receiving emotional support for themselves.
There were no strong predictors of caregiver needs; however, unmet patient needs and caregiver anxiety were modestly associated with unmet needs in caregivers.
Similarly, the SCNS–P&C was administered to 166 lung cancer patient–caregiver dyads in Taiwan.[
Caregiver tasks: A cross-sectional study demonstrated that participation in assisting patients in activities of daily living (ADLs) increased caregiver burden.[
Secondary Appraisal: Resources for Informal Caregivers
The following list captures the resources that caregivers identified in multiple studies as important:
- Recognition by health care providers of the informal caregivers' roles, responsibilities, and challenges.
- Information about treatment plans, goals, anticipated complications or side effects, and likely outcomes.
- Guidance for how to respond to changes in patients' physical and emotional health over the disease trajectory.
- Support in coping with the stress of their role (for which they are most often unprepared and untrained).
- Detailed education about medical and nursing tasks they are expected to perform, such as giving injections, providing wound care, and managing side effects.
Potential Moderators of Caregiver Burden
Factors associated with increased caregiver burden include the following:
- Female gender.
- Age (younger or older with impaired health status).
- Race and ethnicity.
- Lower socioeconomic status.
- Employment status.
- Role strain.
- Site of care.
- Patient characteristics (e.g., level of anxiety, depression, functional status, and quality of life [QOL]).[
13 ][Level of evidence: II]
Female gender
Female gender is an established risk factor for increased burden.[
Age
Family caregivers often feel unprepared, have inadequate knowledge, and receive little guidance from the oncology team for providing care to the cancer patient.[
Younger caregivers must generally juggle work, family responsibilities, and sacrifices involving their social lives. Middle-aged caregivers typically worry about missed workdays, interruptions at work, taking leaves of absence, and reduced productivity.[
Race and ethnicity
In a meta-analysis of 116 empirical studies, Asian American caregivers were found to provide more caregiving hours than were White, African American, and Hispanic caregivers; to use lower levels of formal support services; and to have fewer financial resources, lower levels of education, and higher levels of depression than did the other subgroups.[
A study involving unmet needs and service barriers among Asian American caregivers found that caregivers refused outside help because they "felt too proud to accept it" or "didn't want outsiders coming in"; other barriers included "bureaucracy too complex" or "can't find qualified providers."[
Similarly, Hispanic and African American patients and caregivers underutilize community health resources, including counseling and support groups, home care, residential care, and hospice services. One important reason is that strong family ties may prevent these caregivers from seeking help outside of the family unit.[
Another study analyzed reports of employment loss due to caregiving responsibilities. Results showed that African American and Hispanic caregivers were more likely than White caregivers to reduce their work hours to care for patients. In addition, African American and Hispanic caregivers were reluctant to use formal nursing home services for their loved ones. The decision to reduce work hours rather than place a relative in a nursing home was associated with increased psychological, social, and financial burden.[
Socioeconomic status
Substantial out-of-pocket costs involved in caregiving can create financial strain for the families of patients with cancer. Low personal and household incomes and limited financial resources may also place families at risk of treatment noncompliance or making treatment-related decisions on the basis of income.[
In a secondary analysis of longitudinal data (at baseline, 4–6 weeks, and 3 months) collected during the Improving Communication in Older Cancer Patients and their Caregivers trial, investigators assessed caregiver burden in 414 caregivers of older patients with advanced cancer.[
Employment
Informal caregiving is known to impose economic burdens on families. One study analyzed data from 458 cancer survivors who responded to the U.S. Medical Expenditure Panel Survey (MEPS) Experiences with Cancer Survivorship Survey (ECSS) and from 4,706 cancer survivors who responded to the LIVESTRONG 2012 Survey for People Affected by Cancer (SPAC). Results demonstrated that 25% of those responding to the MEPS ECSS and 29% of those responding to the SPAC reported that their caregivers made extended employment changes, including taking paid or unpaid time off and/or making changes in hours, duties, or employment status.[
Some research has shown an incremental increase in the economic burden of caregiving, assessed from disease and demographic characteristics. A study of 78 caregivers of women with advanced breast cancer showed that loss of productivity (absenteeism and reduced productivity at work) was greater for caregivers of women with progressive disease than for caregivers of those who were free of disease.[
The Family and Medical Leave Act of 1993 (FMLA) was designed to give employees the option of taking time off from work for their own serious medical condition or that of a relative without losing their jobs or benefits.[
Role strain
Role strain is experienced when the perceived rights, duties, and behaviors of one socially defined role (e.g., employee) conflict with the rights, duties, and behaviors of a different role (e.g., student). The multiple roles performed by caregivers of cancer patients can compete for caregivers' physical and emotional resources. A study of 457 middle-aged caregivers showed that the more social roles a caregiver performed, the more likely the caregiver was to experience stress and negative affect.[
Site of care
Cancer care is provided in multiple physical locations that vary in their ability to provide support services for caregivers. Thus, site of care may be considered a risk factor for caregiver burden. This claim is supported by the results of a qualitative interview study of 12 patients and 12 caregivers about the challenges faced in transitioning from hospital to home.[
- Ongoing concerns related to disease and its treatment.
- Needing timely help.
- Resuming control and normality.
- Appreciating the care transition.
An independent study of dyads demonstrated that the transition to home is very stressful because of the need to deal with symptoms, and uncertainty about prognosis and disease progression.[
Unplanned changes in sites of care, such as hospital readmission, also place increased demands on caregivers. A total of 129 dyads of older adults with cancer and their family caregivers were studied to determine factors for unplanned hospital admissions.[
Patient characteristics
Patient characteristics may also influence caregiver burden. In a cross-sectional study of 441 older patient-caregiver dyads with advanced cancer, patients with higher levels of anxiety and depression, worse functional status, and poorer QOL were associated with increased reports of caregiver burden, regardless of time spent caregiving.[
Similarly, in a cross-sectional study of 172 dyads of patients with advanced cancer and their caregivers, caregivers of patients admitted to an acute palliative care unit reported worse stress burden and mental health than caregivers of patients receiving outpatient supportive care.[
References:
- Lazarus RS, Folkman S: Stress, Appraisal, and Coping. Springer Publishing Co, 1984.
- Ream E, Pedersen VH, Oakley C, et al.: Informal carers' experiences and needs when supporting patients through chemotherapy: a mixed method study. Eur J Cancer Care (Engl) 22 (6): 797-806, 2013.
- Badr H, Herbert K, Reckson B, et al.: Unmet needs and relationship challenges of head and neck cancer patients and their spouses. J Psychosoc Oncol 34 (4): 336-46, 2016 Jul-Aug.
- Wheelwright S, Darlington AS, Hopkinson JB, et al.: A systematic review and thematic synthesis of quality of life in the informal carers of cancer patients with cachexia. Palliat Med 30 (2): 149-60, 2016.
- Girgis A, Lambert S, Lecathelinais C: The supportive care needs survey for partners and caregivers of cancer survivors: development and psychometric evaluation. Psychooncology 20 (4): 387-93, 2011.
- Oberoi DV, White V, Jefford M, et al.: Caregivers' information needs and their 'experiences of care' during treatment are associated with elevated anxiety and depression: a cross-sectional study of the caregivers of renal cancer survivors. Support Care Cancer 24 (10): 4177-86, 2016.
- Sklenarova H, Krümpelmann A, Haun MW, et al.: When do we need to care about the caregiver? Supportive care needs, anxiety, and depression among informal caregivers of patients with cancer and cancer survivors. Cancer 121 (9): 1513-9, 2015.
- Chen SC, Chiou SC, Yu CJ, et al.: The unmet supportive care needs-what advanced lung cancer patients' caregivers need and related factors. Support Care Cancer 24 (7): 2999-3009, 2016.
- Hsu T, Loscalzo M, Ramani R, et al.: Factors associated with high burden in caregivers of older adults with cancer. Cancer 120 (18): 2927-35, 2014.
- Lund L, Ross L, Petersen MA, et al.: Cancer caregiving tasks and consequences and their associations with caregiver status and the caregiver's relationship to the patient: a survey. BMC Cancer 14: 541, 2014.
- Ge L, Mordiffi SZ: Factors Associated With Higher Caregiver Burden Among Family Caregivers of Elderly Cancer Patients: A Systematic Review. Cancer Nurs 40 (6): 471-478, 2017 Nov/Dec.
- Stetz KM: Caregiving demands during advanced cancer. The spouse's needs. Cancer Nurs 10 (5): 260-8, 1987.
- Semere W, Althouse AD, Rosland AM, et al.: Poor patient health is associated with higher caregiver burden for older adults with advanced cancer. J Geriatr Oncol 12 (5): 771-778, 2021.
- Kim Y, van Ryn M, Jensen RE, et al.: Effects of gender and depressive symptoms on quality of life among colorectal and lung cancer patients and their family caregivers. Psychooncology 24 (1): 95-105, 2015.
- Decadt I, Laenen A, Celus J, et al.: Caregiver distress and quality of life in primary caregivers of oncology patients in active treatment and follow-up. Eur J Cancer Care (Engl) 30 (3): e13399, 2021.
- Schrank B, Ebert-Vogel A, Amering M, et al.: Gender differences in caregiver burden and its determinants in family members of terminally ill cancer patients. Psychooncology 25 (7): 808-14, 2016.
- Scherbring M: Effect of caregiver perception of preparedness on burden in an oncology population. Oncol Nurs Forum 29 (6): E70-6, 2002.
- Given CW, Stommel M, Given B, et al.: The influence of cancer patients' symptoms and functional states on patients' depression and family caregivers' reaction and depression. Health Psychol 12 (4): 277-85, 1993.
- Schulz R, Beach SR: Caregiving as a risk factor for mortality: the Caregiver Health Effects Study. JAMA 282 (23): 2215-9, 1999.
- Cameron JI, Franche RL, Cheung AM, et al.: Lifestyle interference and emotional distress in family caregivers of advanced cancer patients. Cancer 94 (2): 521-7, 2002.
- Given B, Sherwood PR: Family care for the older person with cancer. Semin Oncol Nurs 22 (1): 43-50, 2006.
- Pinquart M, Sörensen S: Ethnic differences in stressors, resources, and psychological outcomes of family caregiving: a meta-analysis. Gerontologist 45 (1): 90-106, 2005.
- Li H: Barriers to and unmet needs for supportive services: experiences of Asian-American caregivers. J Cross Cult Gerontol 19 (3): 241-60, 2004.
- Ngo-Metzger Q, McCarthy EP, Burns RB, et al.: Older Asian Americans and Pacific Islanders dying of cancer use hospice less frequently than older white patients. Am J Med 115 (1): 47-53, 2003.
- Guarnaccia PJ, Parra P: Ethnicity, social status, and families' experiences of caring for a mentally ill family member. Community Ment Health J 32 (3): 243-60, 1996.
- Cox C, Monk A: Strain among caregivers: comparing the experiences of African American and Hispanic caregivers of Alzheimer's relatives. Int J Aging Hum Dev 43 (2): 93-105, 1996.
- Covinsky KE, Eng C, Lui LY, et al.: Reduced employment in caregivers of frail elders: impact of ethnicity, patient clinical characteristics, and caregiver characteristics. J Gerontol A Biol Sci Med Sci 56 (11): M707-13, 2001.
- Hayman JA, Langa KM, Kabeto MU, et al.: Estimating the cost of informal caregiving for elderly patients with cancer. J Clin Oncol 19 (13): 3219-25, 2001.
- Xu H, Kadambi S, Mohile SG, et al.: Caregiving burden of informal caregivers of older adults with advanced cancer: The effects of rurality and education. J Geriatr Oncol 12 (7): 1015-1021, 2021.
- de Moor JS, Dowling EC, Ekwueme DU, et al.: Employment implications of informal cancer caregiving. J Cancer Surviv 11 (1): 48-57, 2017.
- Mazanec SR, Daly BJ, Douglas SL, et al.: Work productivity and health of informal caregivers of persons with advanced cancer. Res Nurs Health 34 (6): 483-95, 2011.
- Grunfeld E, Coyle D, Whelan T, et al.: Family caregiver burden: results of a longitudinal study of breast cancer patients and their principal caregivers. CMAJ 170 (12): 1795-801, 2004.
- Lambert-Obry V, Gouault-Laliberté A, Castonguay A, et al.: Real-world patient- and caregiver-reported outcomes in advanced breast cancer. Curr Oncol 25 (4): e282-e290, 2018.
- Van Houtven CH, Ramsey SD, Hornbrook MC, et al.: Economic burden for informal caregivers of lung and colorectal cancer patients. Oncologist 15 (8): 883-93, 2010.
- Siefert ML, Williams AL, Dowd MF, et al.: The caregiving experience in a racially diverse sample of cancer family caregivers. Cancer Nurs 31 (5): 399-407, 2008 Sep-Oct.
- Li C, Zeliadt SB, Hall IJ, et al.: Burden among partner caregivers of patients diagnosed with localized prostate cancer within 1 year after diagnosis: an economic perspective. Support Care Cancer 21 (12): 3461-9, 2013.
- Chen ML: The Growing Costs and Burden of Family Caregiving of Older Adults: A Review of Paid Sick Leave and Family Leave Policies. Gerontologist 56 (3): 391-6, 2016.
- Kim Y, Baker F, Spillers RL, et al.: Psychological adjustment of cancer caregivers with multiple roles. Psychooncology 15 (9): 795-804, 2006.
- Fenton ATHR, Keating NL, Ornstein KA, et al.: Comparing adult-child and spousal caregiver burden and potential contributors. Cancer 128 (10): 2015-2024, 2022.
- Ang WH, Lang SP, Ang E, et al.: Transition journey from hospital to home in patients with cancer and their caregivers: a qualitative study. Support Care Cancer 24 (10): 4319-26, 2016.
- Rocío L, Rojas EA, González MC, et al.: Experiences of patient-family caregiver dyads in palliative care during hospital-to-home transition process. Int J Palliat Nurs 23 (7): 332-339, 2017.
- Geddie PI, Wochna Loerzel V, Norris AE: Family Caregiver Knowledge, Patient Illness Characteristics, and Unplanned Hospital Admissions in Older Adults With Cancer. Oncol Nurs Forum 43 (4): 453-63, 2016.
- Tanco K, Prado B, Qian Y, et al.: A Comparison of Caregiver Burden of Patients with Advanced Cancer in Different Palliative Cancer Care Settings. J Palliat Med 24 (12): 1766-1775, 2021.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.