Intraocular (Uveal) Melanoma Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Intraocular (Uveal) Melanoma
Intraocular melanoma is a disease in which malignant (cancer) cells form in the tissues of the eye.
Intraocular melanoma begins in the middle of three layers of the wall of the eye. The outer layer includes the white sclera (the "white of the eye") and the clear cornea at the front of the eye. The inner layer has a lining of nerve tissue, called the retina, which senses light and sends images along the optic nerve to the brain.
The middle layer, where intraocular melanoma forms, is called the uvea or uveal tract, and has three main parts:
| Iris
The iris is the colored area at the front of the eye (the "eye color"). It can be seen through the clear cornea. The pupil is in the center of the iris, and it changes size to let more or less light into the eye. Intraocular melanoma of the iris is usually a small tumor that grows slowly and rarely spreads to other parts of the body. |
| Ciliary body
The ciliary body is a ring of tissue with muscle fibers that change the shape of the lens. It is found behind the iris. Changes in the shape of the lens help the eye focus. The ciliary body also makes the clear fluid that fills the space between the cornea and the iris. Intraocular melanoma of the ciliary body is often larger and more likely to spread to other parts of the body than intraocular melanoma of the iris. |
| Choroid
The choroid is a layer of blood vessels that bring oxygen and nutrients to the eye. Most intraocular melanomas begin in the choroid. Intraocular melanoma of the choroid is often larger and more likely to spread to other parts of the body than intraocular melanoma of the iris. |

Anatomy of the eye, showing the outside and inside of the eye including the sclera, cornea, iris, ciliary body, choroid, retina, vitreous humor, and optic nerve. The vitreous humor is a liquid that fills the center of the eye.
Intraocular melanoma is a rare cancer that forms from cells that make melanin in the iris, ciliary body, and choroid. It is the most common eye cancer in adults.
Being older and having fair skin may increase the risk of intraocular melanoma.
Anything that increases a person's chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop intraocular melanoma, and it will develop in some people who don't have any known risk factors. Talk with your doctor if you think you may be at risk.
Risk factors for intraocular melanoma include:
- Having a fair complexion, which includes:
- Fair skin that freckles and burns easily, does not tan, or tans poorly.
- Blue or green or other light-colored eyes.
- Older age.
- Being White.
Signs and symptoms of intraocular melanoma may include blurred vision or a dark spot on the iris.
Intraocular melanoma may not cause early signs or symptoms. It is sometimes found during a regular eye exam when the doctor dilates the pupil and looks into the eye. These and other signs and symptoms may be caused by intraocular melanoma or by other conditions. Check with your doctor if you have any of the following symptoms that do not go away:
- Blurred vision or other change in vision.
- Floaters (spots that drift in your field of vision) or flashes of light.
- A dark spot on the iris.
- A change in the size or shape of the pupil.
- A change in the position of the eyeball in the eye socket.
Tests that examine the eye are used to diagnose intraocular melanoma.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Eye exam with dilated pupil: An exam of the eye in which the pupil is dilated (enlarged) with medicated eye drops to allow the doctor to look through the lens and pupil to the retina. The inside of the eye, including the retina and the optic nerve, is checked. Pictures may be taken over time to keep track of changes in the size of the tumor. There are several types of eye exams:
- Ophthalmoscopy: An exam of the inside of the back of the eye to check the retina and optic nerve using a small magnifying lens and a light.
- Slit-lamp biomicroscopy: An exam of the inside of the eye to check the retina, optic nerve, and other parts of the eye using a strong beam of light and a microscope.
- Gonioscopy: An exam of the front part of the eye between the cornea and iris. A special instrument is used to see if the area where fluid drains out of the eye is blocked.
- Ultrasound exam of the eye: A procedure in which high-energy sound waves (ultrasound) are bounced off the internal tissues of the eye to make echoes. Eye drops are used to numb the eye, and a small probe that sends and receives sound waves is placed gently on the surface of the eye. The echoes make a picture of the inside of the eye, and the distance from the cornea to the retina is measured. The picture, called a sonogram, shows on the screen of the ultrasound monitor.
- High-resolution ultrasound biomicroscopy: A procedure in which high-energy sound waves (ultrasound) are bounced off the internal tissues of the eye to make echoes. Eye drops are used to numb the eye, and a small probe that sends and receives sound waves is placed gently on the surface of the eye. The echoes make a more detailed picture of the inside of the eye than a regular ultrasound. The tumor is checked for its size, shape, and thickness, and for signs that the tumor has spread to nearby tissue.
- Transillumination of the globe and iris: An exam of the iris, cornea, lens, and ciliary body with a light placed on either the upper or lower lid.
- Fluorescein angiography: A procedure to look at blood vessels and the flow of blood inside the eye. An orange fluorescent dye (fluorescein) is injected into a blood vessel in the arm and goes into the bloodstream. As the dye travels through blood vessels of the eye, a special camera takes pictures of the retina and choroid to find any areas that are blocked or leaking.
- Indocyanine green angiography: A procedure to look at blood vessels in the choroid layer of the eye. A green dye (indocyanine green) is injected into a blood vessel in the arm and goes into the bloodstream. As the dye travels through blood vessels of the eye, a special camera takes pictures of the retina and choroid to find any areas that are blocked or leaking.
- Ocular coherence tomography: An imaging test that uses light waves to take cross-section pictures of the retina, and sometimes the choroid, to see if there is swelling or fluid beneath the retina.
A biopsy of the tumor is rarely needed to diagnose intraocular melanoma.
A biopsy is the removal of cells or tissues so they can be viewed under a microscope by a pathologist to check for signs of cancer. Rarely, a biopsy of the tumor is needed to diagnose intraocular melanoma. Tissue that is removed during a biopsy or surgery to remove the tumor may be tested to get more information about prognosis and which treatment options are best.
The following tests may be done on the sample of tissue:
- Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of tissue are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
- Gene expression profiling: A laboratory test that identifies all of the genes in a cell or tissue that are making (expressing) messenger RNA. Messenger RNA molecules carry the genetic information that is needed to make proteins from the DNA in the cell nucleus to the protein-making machinery in the cell cytoplasm.
A biopsy may result in retinal detachment (the retina separates from other tissues in the eye). This can be repaired by surgery.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on:
- How the melanoma cells look under a microscope.
- The size and thickness of the tumor.
- Whether the tumor is in the iris, ciliary body, or choroid part of the eye.
- Whether the tumor has spread within the eye or to other places in the body.
- Whether there are certain changes in the genes linked to intraocular melanoma.
- The patient's age and general health.
- Whether the tumor has recurred (come back) after treatment.
Stages of Intraocular (Uveal) Melanoma
After intraocular melanoma has been diagnosed, tests are done to find out if cancer cells have spread to other parts of the body.
The process used to find out if cancer has spread to other parts of the body is called staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
The following tests and procedures may be used in the staging process:
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Liver function tests: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by the liver. A higher-than-normal amount of a substance can be a sign the cancer has spread to the liver.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs, such as the liver, and make echoes. The echoes form a picture of body tissues called a sonogram.
- Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body, such as the liver. This procedure is also called nuclear magnetic resonance imaging (NMRI).
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the chest, abdomen, or pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
- PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A very small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. Sometimes a PET scan and a CT scan are done at the same time. If there is any cancer, this increases the chance that it will be found.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
If intraocular melanoma spreads to the optic nerve or nearby tissue of the eye socket, it is called extraocular extension.
Cancer may spread from where it began to other parts of the body.
When cancer spreads to another part of the body, it is called metastasis. Cancer cells break away from where they began (the primary tumor) and travel through the lymph system or blood.
- Lymph system. The cancer gets into the lymph system, travels through the lymph vessels, and forms a tumor (metastatic tumor) in another part of the body.
- Blood. The cancer gets into the blood, travels through the blood vessels, and forms a tumor (metastatic tumor) in another part of the body.
The metastatic tumor is the same type of cancer as the primary tumor. For example, if intraocular melanoma spreads to the liver, the cancer cells in the liver are actually intraocular melanoma cells. The disease is metastatic intraocular melanoma, not liver cancer.
The following sizes are used to describe intraocular melanoma and plan treatment:
Small
The tumor is 5 to 16 millimeters in diameter and from 1 to 3 millimeters thick. 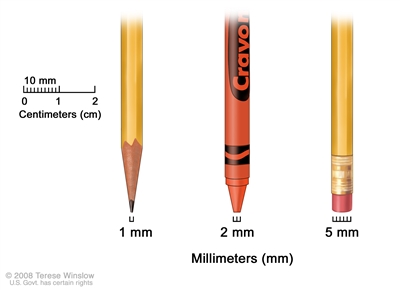
Millimeters (mm). A sharp pencil point is about 1 mm, a new crayon point is about 2 mm, and a new pencil eraser is about 5 mm.
Medium
The tumor is 16 millimeters or smaller in diameter and from 3.1 to 8 millimeters thick.
Large
The tumor is:
- more than 8 millimeters thick and any diameter; or
- at least 2 millimeters thick and more than 16 millimeters in diameter.
Though most intraocular melanoma tumors are raised, some are flat. These diffuse tumors grow widely across the uvea.
There is no staging system for intraocular melanoma of the iris.
The following stages are used for intraocular melanoma of the ciliary body and choroid:
Intraocular melanoma of the ciliary body and choroid has four size categories. The category depends on how wide and thick the tumor is. Category 1 tumors are the smallest, and category 4 tumors are the largest.
Category 1:
- The tumor is not more than 12 millimeters wide and not more than 3 millimeters thick; or
- the tumor is not more than 9 millimeters wide and 3.1 to 6 millimeters thick.
Category 2:
- The tumor is 12.1 to 18 millimeters wide and not more than 3 millimeters thick; or
- the tumor is 9.1 to 15 millimeters wide and 3.1 to 6 millimeters thick; or
- the tumor is not more than 12 millimeters wide and 6.1 to 9 millimeters thick.
Category 3:
- The tumor is 15.1 to 18 millimeters wide and 3.1 to 6 millimeters thick; or
- the tumor is 12.1 to 18 millimeters wide and 6.1 to 9 millimeters thick; or
- the tumor is not more than 18 millimeters wide and 9.1 to 12 millimeters thick; or
- the tumor is not more than 15 millimeters wide and 12.1 to 15 millimeters thick.
Category 4:
- The tumor is more than 18 millimeters wide and may be any thickness; or
- the tumor is 15.1 to 18 millimeters wide and more than 12 millimeters thick; or
- the tumor is not more than 15 millimeters wide and more than 15 millimeters thick.
Stage I
In stage I, the tumor is size category 1 and is in the choroid only.
Stage II
Stage II is divided into stages IIA and IIB.
- In stage IIA, the tumor:
- is size category 1 and has spread to the ciliary body; or
- is size category 1 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor may have spread to the ciliary body; or
- is size category 2 and is in the choroid only.
- In stage IIB, the tumor:
- is size category 2 and has spread to the ciliary body; or
- is size category 3 and is in the choroid only.
Stage III
Stage III is divided into stages IIIA, IIIB, and IIIC.
- In stage IIIA, the tumor:
- is size category 2 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor may have spread to the ciliary body; or
- is size category 3 and has spread to the ciliary body; or
- is size category 3 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor has not spread to the ciliary body; or
- is size category 4 and is in the choroid only.
- In stage IIIB, the tumor:
- is size category 3 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor has spread to the ciliary body; or
- is size category 4 and has spread to the ciliary body; or
- is size category 4 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor has not spread to the ciliary body.
- In stage IIIC, the tumor:
- is size category 4 and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is not more than 5 millimeters thick. The tumor has spread to the ciliary body; or
- may be any size and has spread through the sclera to the outside of the eyeball. The part of the tumor outside the eyeball is more than 5 millimeters thick.
Stage IV
In stage IV, the tumor may be any size and has spread:
- to one or more nearby lymph nodes or to the eye socket separate from the primary tumor; or
- to other parts of the body, such as the liver, lung, bone, brain, or tissue under the skin.
Intraocular melanoma can recur (come back) after it has been treated.
The melanoma may come back in the eye or in other parts of the body.
Treatment Option Overview
There are different types of treatment for patients with intraocular melanoma.
Different types of treatment are available for patients with intraocular melanoma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
The following types of treatment are used:
Surgery
Surgery is the most common treatment for intraocular melanoma. The following types of surgery may be used:
- Resection: Surgery to remove the tumor and a small amount of healthy tissue around it.
- Enucleation: Surgery to remove the eye and part of the optic nerve. This is done if vision cannot be saved and the tumor is large, has spread to the optic nerve, or causes high pressure inside the eye. After surgery, the patient is usually fitted for an artificial eye to match the size and color of the other eye.
- Exenteration: Surgery to remove the eye and eyelid, and muscles, nerves, and fat in the eye socket. After surgery, the patient may be fitted for an artificial eye to match the size and color of the other eye or a facial prosthesis.
Watchful waiting
Watchful waiting is closely monitoring a patient's condition without giving any treatment until signs or symptoms appear or change. Pictures are taken over time to keep track of changes in the size of the tumor and how fast it is growing.
Watchful waiting is used for patients who do not have signs or symptoms, and the tumor is not growing. It is also used when the tumor is in the only eye with useful vision.
Radiation therapy
Radiation therapy is a cancer treatment that uses high-energy x-rays or other types of radiation to kill cancer cells or keep them from growing. There are two types of radiation therapy:
- External radiation therapy uses a machine outside the body to send radiation toward the cancer. Certain ways of giving radiation therapy can help keep radiation from damaging nearby healthy tissue. These types of external radiation therapy include:
- Charged-particle external-beam radiation therapy is a type of external-beam radiation therapy. A special radiation therapy machine aims tiny, invisible particles, called protons or helium ions, at the cancer cells to kill them with little damage to nearby normal tissues. Charged-particle radiation therapy uses a different type of radiation than the x-ray type of radiation therapy.
- Gamma Knife therapy is a type of stereotactic radiosurgery used for some melanomas. This treatment can be given in one treatment. It aims tightly focused gamma rays directly at the tumor so there is little damage to healthy tissue. Gamma Knife therapy does not use a knife to remove the tumor and is not an operation.
- Internal radiation therapy uses a radioactive substance sealed in needles, seeds, wires, or catheters that are placed directly into or near the cancer. Certain ways of giving radiation therapy can help keep radiation from damaging healthy tissue. This type of internal radiation therapy may include:
- Localized plaque radiation therapy is a type of internal radiation therapy that may be used for tumors of the eye. Radioactive seeds are attached to one side of a disk, called a plaque, and placed directly on the outside wall of the eye near the tumor. The side of the plaque with the seeds on it faces the eyeball, aiming radiation at the tumor. The plaque helps protect other nearby tissue from the radiation.
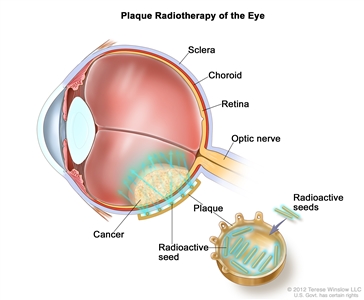
Plaque radiotherapy is a type of radiation therapy used to treat eye cancer. Radioactive seeds are attached to one side of a thin piece of metal (usually gold) called a plaque. The plaque is sewn onto the outside wall of the eye near the tumor. The seeds give off radiation which kills the cancer. The plaque is removed at the end of treatment, which usually lasts for several days.
The way the radiation therapy is given depends on the type and stage of the cancer being treated. External and internal radiation therapy are used to treat intraocular melanoma.
Photocoagulation
Photocoagulation is a procedure that uses laser light to destroy blood vessels that bring nutrients to the tumor, causing the tumor cells to die. Photocoagulation may be used to treat small tumors. This is also called light coagulation.
Thermotherapy
Thermotherapy is the use of heat from a laser to destroy cancer cells and shrink the tumor.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the
Treatment for intraocular (uveal) melanoma may cause side effects.
For information about side effects caused by treatment for cancer, visit our
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's
Follow-up care may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.