Lymphedema (PDQ®): Supportive care - Health Professional Information [NCI]
Overview
Lymphedema occurs when disruption of normal lymphatic drainage leads to accumulation of protein-rich lymph fluid in the interstitial space. Cancer survivors who experience lymphedema report poor physical functioning, impaired ability to engage in normal activities of daily living, and increased psychological distress.[
Estimates of the prevalence of lymphedema vary widely due to differences in the type of cancer, measurement methods, diagnostic criteria, and timing of evaluations relative to cancer diagnosis and treatment. In a survey conducted in 2006 and 2010, 6,593 cancer survivors were asked to identify ongoing concerns. Approximately 20% of respondents reported concerns related to lymphedema. Of these individuals, 50% to 60% reported receiving care for lymphedema.[
Lymphedema is a common delayed effect of cancer treatment that negatively impacts survivors' quality of life. This summary reviews the anatomy of the lymphatic system, the pathophysiology of lymphedema secondary to cancer, and epidemiology. The summary also provides clinicians with information related to risk factors, diagnosis, prevention, and treatment. The summary does not deal with congenital lymphedema or lymphedema not related to cancer.
In this summary, unless otherwise stated, evidence and practice issues as they relate to adults are discussed. The evidence and application to practice related to children may differ significantly from information related to adults. When specific information about the care of children is available, it is summarized under its own heading.
Anatomy of the Lymphatic System
The human lymphatic system generally includes superficial or primary lymphatic vessels that form a complex dermal network of capillary-like channels. Primary lymphatic vessels lack muscular walls and do not have valves. They drain into larger, secondary lymphatic vessels located in the subdermal space. Secondary lymphatic vessels run parallel to the superficial veins and drain into deeper lymphatic vessels located in the subcutaneous fat adjacent to the fascia. Unlike the primary vessels, the secondary and deeper lymphatic vessels have muscular walls and numerous valves to accomplish active and unidirectional lymphatic flow.
An intramuscular system of lymphatic vessels that parallels the deep arteries and drains the muscular compartment, joints, and synovium also exists. The superficial and deep lymphatic systems probably function independently, except in abnormal states, although there is evidence that they communicate near lymph nodes.[
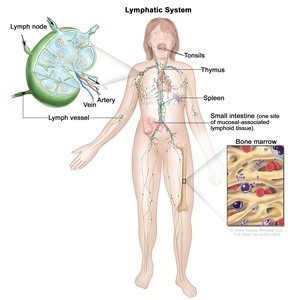
The lymph system is part of the body's immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, adenoids (not shown), thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph tissue is also found in many other parts of the body, including the small intestine.
Pathophysiology of Lymphedema
Body fluids can be discussed in terms of their composition and the specific fluid compartment where they are located. Intracellular fluid includes all fluid enclosed by the plasma membranes of cells. Extracellular fluid (ECF) surrounds all cells in the body. ECF has two primary constituents: intravascular plasma and the interstitial fluid that surrounds all cells not in the plasma. Lymphedema is the abnormal accumulation of protein-rich fluid in the interstitial space that is accompanied by inflammation and, eventually, fibrosis.
The formation of interstitial fluid comes from the movement of intravascular fluid across the capillary membranes due to arteriolar blood pressure. Much of the interstitial fluid returns to the intravascular fluid via the postcapillary venules. The dynamics of fluid production are influenced by arterial and venous hydrostatic pressures, tissue pressure, oncotic pressures of the intravascular and interstitial fluid, and membrane permeability. Normally, the dynamics favor a net gain of interstitial fluid, with the excess removed via lymphatic channels. Because lymphatic vessels often lack a basement membrane, they can resorb molecules too large for venous uptake as well. In short, the lymphatic system controls the pressure, volume, and composition of the interstitial fluid.
Lymphatic obstruction leads to increased interstitial fluid, which often contains large proteins and cellular debris. Through mechanisms not fully understood, the increased interstitial fluid induces inflammation, destruction or sclerosis of the lymphatic vessels, fibrosis, and, ultimately, adipose tissue hypertrophy.
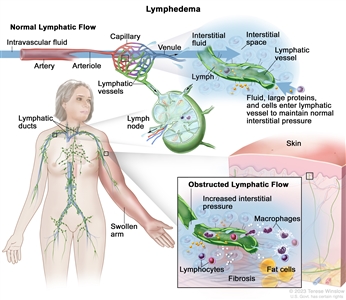
The lymphatic vessels normally maintain normal interstitial pressures by removing the excess interstitial fluid that results from the imbalance between the intravascular fluid that enters from the arterioles and exits into the venules. Large proteins and cells that cannot exit the interstitial space through the venules leave the interstitial fluid through the lymphatic vessels. As the lymph moves through the lymphatic vessels, it passes through lymph nodes and eventually into one of two lymphatic ducts that empty into a large vein near the heart. In lymphedema, the flow of lymph through the lymphatic vessels is disrupted or blocked. This leads to increased interstitial pressure and an accumulation of interstitial fluid, large proteins, and cellular debris in the interstitial space, which induces inflammation. The inflammation may cause further damage to the lymphatic vessels. The macrophages and lymphocytes release inflammatory markers, which causes fibrosis, fat cell hypertrophy, and the classical sign of swelling. Lymphedema may be caused by cancer or cancer treatment.
Epidemiology and Risk Factors
Accurate estimates of the incidence and prevalence of lymphedema are difficult to provide, due in part to differences in the definition of lymphedema (e.g., patient self-reports vs. objective volume measurements) and the timing of assessment for lymphedema relative to cancer treatment. Other factors are differences in surgical techniques related to the type of lymph node dissection or the total dose, fractions, and field of radiation administered.
Common risk factors for developing lymphedema include the following:
- Extent of local surgery.
- Anatomical location of lymph node dissection.
- Radiation to lymph nodes.
- Localized infection or delayed wound healing.
- Tumor causing lymphatic obstruction of the anterior cervical, thoracic, axillary, pelvic, or abdominal nodes.
- Intrapelvic or intra-abdominal tumors that involve or directly compress lymphatic vessels and/or the cisterna chyli and thoracic duct.
- Having a higher disease stage.
- Overweight (body mass index [BMI] ≥25 kg/m2) or obesity (BMI ≥30 kg/m2).[
9 ] - Black race and Hispanic ethnicity.[
10 ] - Rurality.[
10 ]
References:
- Ridner SH: Quality of life and a symptom cluster associated with breast cancer treatment-related lymphedema. Support Care Cancer 13 (11): 904-11, 2005.
- Dunberger G, Lindquist H, Waldenström AC, et al.: Lower limb lymphedema in gynecological cancer survivors--effect on daily life functioning. Support Care Cancer 21 (11): 3063-70, 2013.
- Zhang X, McLaughlin EM, Krok-Schoen JL, et al.: Association of Lower Extremity Lymphedema With Physical Functioning and Activities of Daily Living Among Older Survivors of Colorectal, Endometrial, and Ovarian Cancer. JAMA Netw Open 5 (3): e221671, 2022.
- Pyszel A, Malyszczak K, Pyszel K, et al.: Disability, psychological distress and quality of life in breast cancer survivors with arm lymphedema. Lymphology 39 (4): 185-92, 2006.
- Gjorup CA, Groenvold M, Hendel HW, et al.: Health-related quality of life in melanoma patients: Impact of melanoma-related limb lymphoedema. Eur J Cancer 85: 122-132, 2017.
- Beckjord EB, Reynolds KA, van Londen GJ, et al.: Population-level trends in posttreatment cancer survivors' concerns and associated receipt of care: results from the 2006 and 2010 LIVESTRONG surveys. J Psychosoc Oncol 32 (2): 125-51, 2014.
- Paskett ED, Le-Rademacher J, Oliveri JM, et al.: A randomized study to prevent lymphedema in women treated for breast cancer: CALGB 70305 (Alliance). Cancer 127 (2): 291-299, 2021.
- Horsley JS, Styblo T: Lymphedema in the postmastectomy patient. In: Bland KI, Copeland EM, eds.: The Breast: Comprehensive Management of Benign and Malignant Diseases. Saunders, 1991, pp 701-6.
- McLaughlin SA, Brunelle CL, Taghian A: Breast Cancer-Related Lymphedema: Risk Factors, Screening, Management, and the Impact of Locoregional Treatment. J Clin Oncol 38 (20): 2341-2350, 2020.
- Montagna G, Zhang J, Sevilimedu V, et al.: Risk Factors and Racial and Ethnic Disparities in Patients With Breast Cancer-Related Lymphedema. JAMA Oncol 8 (8): 1195-1200, 2022.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.