Myelodysplastic Syndromes Treatment (PDQ®): Treatment - Patient Information [NCI]
General Information About Myelodysplastic Syndromes
Myelodysplastic syndromes are a group of cancers in which immature blood cells in the bone marrow do not mature or become healthy blood cells.
In a healthy person, the bone marrow makes blood stem cells (immature cells) that become mature blood cells over time.
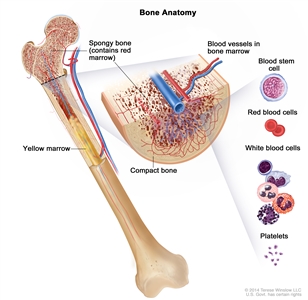
Anatomy of the bone. The bone is made up of compact bone, spongy bone, and bone marrow. Compact bone makes up the outer layer of the bone. Spongy bone is found mostly at the ends of bones and contains red marrow. Bone marrow is found in the center of most bones and has many blood vessels. There are two types of bone marrow: red and yellow. Red marrow contains blood stem cells that can become red blood cells, white blood cells, or platelets. Yellow marrow is made mostly of fat.
A blood stem cell may become a lymphoid stem cell or a myeloid stem cell. A lymphoid stem cell becomes a white blood cell. A myeloid stem cell becomes one of three types of mature blood cells:
- Red blood cells that carry oxygen and other substances to all tissues of the body.
- Platelets that form blood clots to stop bleeding.
- Granulocytes, which are white blood cells that help fight infection and disease.
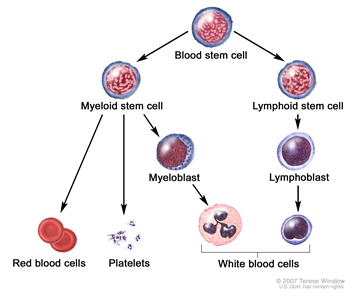
Blood cell development. A blood stem cell goes through several steps to become a red blood cell, platelet, or white blood cell.
In a patient with a myelodysplastic syndrome, the blood stem cells (immature cells) do not become mature red blood cells, white blood cells, or platelets in the bone marrow. These immature blood cells, called blasts, do not work the way they should and either die in the bone marrow or soon after they go into the blood. This leaves less room for healthy white blood cells, red blood cells, and platelets to form in the bone marrow. When there are fewer healthy blood cells, infection, anemia, or easy bleeding may occur.
The different types of myelodysplastic syndromes are diagnosed based on certain changes in the blood cells and bone marrow.
- Refractory anemia: There are too few red blood cells in the blood and the patient has anemia. The number of white blood cells and platelets is normal.
- Refractory anemia with ring sideroblasts: There are too few red blood cells in the blood and the patient has anemia. The red blood cells have too much iron inside the cell. The number of white blood cells and platelets is normal.
- Refractory anemia with excess blasts: There are too few red blood cells in the blood and the patient has anemia. Five percent to 19% of the cells in the bone marrow are blasts. There also may be changes to the white blood cells and platelets. Refractory anemia with excess blasts may progress to acute myeloid leukemia (AML). For more information, see
Acute Myeloid Leukemia Treatment . - Refractory cytopenia with multilineage dysplasia: There are too few of at least two types of blood cells (red blood cells, platelets, or white blood cells). Less than 5% of the cells in the bone marrow are blasts and less than 1% of the cells in the blood are blasts. If red blood cells are affected, they may have extra iron. Refractory cytopenia may progress to acute myeloid leukemia (AML).
- Refractory cytopenia with unilineage dysplasia: There are too few of one type of blood cell (red blood cells, platelets, or white blood cells). There are changes in 10% or more of two other types of blood cells. Less than 5% of the cells in the bone marrow are blasts and less than 1% of the cells in the blood are blasts.
- Unclassifiable myelodysplastic syndrome: The numbers of blasts in the bone marrow and blood are normal, and the disease is not one of the other myelodysplastic syndromes.
- Myelodysplastic syndrome associated with an isolated del(5q) chromosome abnormality: There are too few red blood cells in the blood and the patient has anemia. Less than 5% of the cells in the bone marrow and blood are blasts. There is a specific change in the chromosome.
- Chronic myelomonocytic leukemia (CMML): For more information, see
Myelodysplastic/Myeloproliferative Neoplasms Treatment .
Age and past treatment with chemotherapy or radiation therapy affect the risk of a myelodysplastic syndrome.
Anything that increases a person's chance of getting a disease is called a risk factor. Not every person with one or more of these risk factors will develop myelodysplastic syndromes, and they will develop in people who don't have any known risk factors. Talk with your doctor if you think you may be at risk. Risk factors for myelodysplastic syndromes include the following:
- Past treatment with chemotherapy or radiation therapy for cancer.
- Being exposed to certain chemicals, including tobacco smoke, pesticides, fertilizers, and solvents such as benzene.
- Being exposed to heavy metals, such as mercury or lead.
The cause of myelodysplastic syndromes in most patients is not known.
Signs and symptoms of a myelodysplastic syndrome include shortness of breath and feeling tired.
Myelodysplastic syndromes often do not cause early signs or symptoms. They may be found during a routine blood test. Signs and symptoms may be caused by myelodysplastic syndromes or by other conditions. Check with your doctor if you have any of the following:
- Shortness of breath.
- Weakness or feeling tired.
- Having skin that is paler than usual.
- Easy bruising or bleeding.
- Petechiae (flat, pinpoint spots under the skin caused by bleeding).
Tests that examine the blood and bone marrow are used to diagnose myelodysplastic syndromes.
In addition to asking about your personal and family health history and doing a physical exam, your doctor may perform the following tests and procedures:
- Complete blood count (CBC) with differential: A procedure in which a sample of blood is drawn and checked for the following:
- The number of red blood cells and platelets.
- The number and type of white blood cells.
- The amount of hemoglobin (the protein that carries oxygen) in the red blood cells.
- The portion of the blood sample made up of red blood cells.
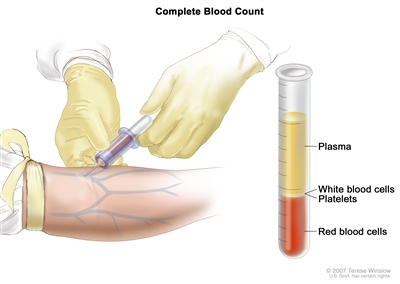
Complete blood count (CBC). Blood is collected by inserting a needle into a vein and allowing the blood to flow into a tube. The blood sample is sent to the laboratory and the red blood cells, white blood cells, and platelets are counted. The CBC is used to test for, diagnose, and monitor many different conditions. - Peripheral blood smear: A procedure in which a sample of blood is checked for changes in the number, type, shape, and size of blood cells and for too much iron in the red blood cells.
- Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of bone marrow or blood are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances, such as vitamin B12 and folate, released into the blood by organs and tissues in the body. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Bone marrow aspiration and biopsy: The removal of bone marrow, blood, and a small piece of bone by inserting a hollow needle into the hipbone or breastbone. A pathologist views the bone marrow, blood, and bone under a microscope to look for abnormal cells.
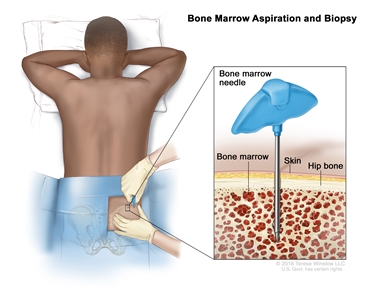
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a long, hollow needle is inserted through the patient's skin and hip bone into the bone marrow. A sample of bone marrow and a small piece of bone are removed for examination under a microscope.The following tests may be done on the sample of tissue that is removed:
- Immunocytochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient's bone marrow. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to the antigen in the sample of the patient's cells, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to tell the difference between myelodysplastic syndromes, leukemia, and other conditions.
- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of leukemia and other blood disorders.
- Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient's blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
- FISH (fluorescence in situ hybridization): A laboratory test used to look at and count genes or chromosomes in cells and tissues. Pieces of DNA that contain fluorescent dyes are made in the laboratory and added to a sample of a patient's cells or tissues. When these dyed pieces of DNA attach to certain genes or areas of chromosomes in the sample, they light up when viewed under a fluorescent microscope. The FISH test is used to help diagnose cancer and help plan treatment.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on the following:
- The number of blast cells in the bone marrow.
- Whether one or more types of blood cells are affected.
- Whether the patient has signs or symptoms of anemia, bleeding, or infection.
- Whether the patient has a low or high risk of leukemia.
- Certain changes in the chromosomes.
- Whether the myelodysplastic syndrome occurred after chemotherapy or radiation therapy for cancer.
- The patient's age and general health.
Treatment Option Overview
There are different types of treatment for patients with myelodysplastic syndromes.
Different types of treatment are available for patients with myelodysplastic syndromes. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment. Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Treatment for myelodysplastic syndromes includes supportive care, drug therapy, and stem cell transplant.
Patients with a myelodysplastic syndrome who have symptoms caused by low blood counts are given supportive care to relieve symptoms and improve quality of life. Drug therapy may be used to slow progression of the disease. Certain patients can be cured with aggressive treatment with chemotherapy followed by stem cell transplant using stem cells from a donor.
The following types of treatment are used:
Supportive care
Supportive care is given to lessen the problems caused by the disease or its treatment. Supportive care may include the following:
- Transfusion therapy
Transfusion therapy (blood transfusion) is a method of giving red blood cells, white blood cells, or platelets to replace blood cells destroyed by disease or treatment. A red blood cell transfusion is given when the red blood cell count is low and signs or symptoms of anemia, such as shortness of breath or feeling very tired, occur. A platelet transfusion is usually given when the patient is bleeding, is having a procedure that may cause bleeding, or when the platelet count is very low.
Patients who receive many blood cell transfusions may have tissue and organ damage caused by the buildup of extra iron. These patients may be treated with iron chelation therapy to remove the extra iron from the blood.
- Erythropoiesis-stimulating agents
Erythropoiesis-stimulating agents (ESAs) may be given to increase the number of mature red blood cells made by the body and to lessen the effects of anemia. Sometimes granulocyte colony-stimulating factor (G-CSF) is given with ESAs to help the treatment work better.
- Antibiotic therapy
Antibiotics may be given to fight infection.
Drug therapy
- Lenalidomide
Patients with myelodysplastic syndrome associated with an isolated del(5q) chromosome abnormality who need frequent red blood cell transfusions may be treated with lenalidomide. Lenalidomide is used to lessen the need for red blood cell transfusions.
- Immunosuppressive therapy
Antithymocyte globulin (ATG) works to suppress or weaken the immune system. It is used to lessen the need for red blood cell transfusions.
- Azacitidine and decitabine
Azacitidine and decitabine are used to treat myelodysplastic syndromes by killing cells that are dividing rapidly. They also help genes that are involved in cell growth to work the way they should. Treatment with azacitidine and decitabine may slow the progression of myelodysplastic syndromes to acute myeloid leukemia.
- Chemotherapy used in acute myeloid leukemia (AML)
Patients with a myelodysplastic syndrome and a high number of blasts in their bone marrow have a high risk of acute leukemia. They may be treated with the same chemotherapy regimen used in patients with acute myeloid leukemia.
Chemotherapy with stem cell transplant
Chemotherapy is given to kill cancer cells. Healthy cells, including blood -forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given back to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
This treatment may not work as well in patients whose myelodysplastic syndrome was caused by past treatment for cancer. 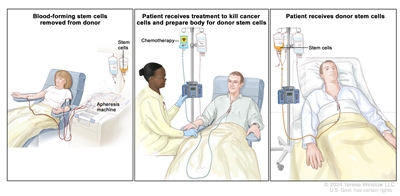
Donor stem cell transplant. (Step 1): Four to five days before donor stem cell collection, the donor receives a medicine to increase the number of stem cells circulating through their bloodstream (not shown). The blood-forming stem cells are then collected from the donor through a large vein in their arm. The blood flows through an apheresis machine that removes the stem cells. The rest of the blood is returned to the donor through a vein in their other arm. (Step 2): The patient receives chemotherapy to kill cancer cells and prepare their body for the donor stem cells. The patient may also receive radiation therapy (not shown). (Step 3): The patient receives an infusion of the donor stem cells.
New types of treatment are being tested in clinical trials.
Information about clinical trials is available from the
Treatment for myelodysplastic syndromes may cause side effects.
For information about side effects caused by treatment for cancer, visit our
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's
Follow-up tests may be needed.
As you go through treatment, you will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your condition has changed or if the cancer has recurred (come back).
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.