Prostate Cancer Treatment (PDQ®): Treatment - Health Professional Information [NCI]
General Information About Prostate Cancer
The median age at diagnosis of prostate cancer is 67 years.[
Many patients—especially those with localized tumors—may die of other illnesses without ever having suffered disability from prostate cancer, even if managed conservatively without an attempt at curative therapy.[
Because diagnostic methods have changed over time, any analysis of survival after treatment of prostate cancer and comparison of the various treatment strategies is complicated by evidence of increasing diagnosis of nonlethal tumors. Nonrandomized comparisons of treatments may be confounded not only by patient selection factors but also by time trends.
For example, a population-based study in Sweden showed that, from 1960 to the late 1980s, before the use of PSA for screening purposes, long-term relative survival rates after the diagnosis of prostate cancer improved substantially as more sensitive methods of diagnosis were introduced. This occurred despite the use of watchful waiting or active surveillance or palliative hormonal treatment as the most common treatment strategies for localized prostate cancer during the entire era (<150 radical prostatectomies per year were performed in Sweden during the late 1980s). The investigators estimated that, if all prostate cancers diagnosed between 1960 and 1964 were of the lethal variety, then at least 33% of cancers diagnosed between 1980 and 1984 were of the nonlethal variety.[
Another issue complicating comparisons of outcomes among nonconcurrent series of patients is the possibility of changes in criteria for the histological diagnosis of prostate cancer.[
Controversy exists about the value of screening, the most appropriate staging evaluation, and the optimal treatment of each stage of the disease.[
Incidence and Mortality
Estimated new cases and deaths from prostate cancer in the United States in 2025:[
- New cases: 313,780.
- Deaths: 35,770.
Anatomy
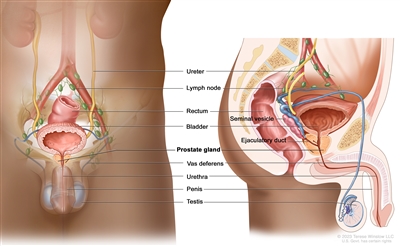
Figure 1. Anatomy of the male reproductive and urinary systems.
Screening
Screening for prostate cancer is controversial. In the United States, most prostate cancers are diagnosed because of screening, either with a PSA blood test or, less frequently, with a digital rectal examination. Randomized trials have yielded conflicting results.[
For a detailed summary of evidence regarding the benefits and harms of screening for prostate cancer, see
Pathology
More than 95% of primary prostate cancers are adenocarcinomas. Prostate adenocarcinomas are frequently multifocal and heterogeneous in patterns of differentiation. Prostatic intraepithelial neoplasia (PIN) (noninvasive atypical epithelial cells within benign-appearing acini) is often present in association with prostatic adenocarcinoma. PIN is subdivided into low grade and high grade. The high-grade form may be a precursor of adenocarcinoma.[
Several rare tumors account for the rest of the cases. These include:
- Small-cell tumors.
- Intralobular acinar carcinomas.
- Ductal carcinomas.
- Clear cell carcinomas.
- Mucinous carcinomas.[
21 ]
Gleason score
The histological grade of prostate adenocarcinomas is usually reported according to one of the variations of the Gleason scoring system, which provides a useful, albeit crude, adjunct to tumor staging in determining prognosis.[
There is evidence that, over time, pathologists have tended to award higher Gleason scores to the same histological patterns, a phenomenon sometimes termed grade inflation.[
Molecular markers
A number of tumor markers are associated with the outcome of patients with prostate cancer, including:[
- Markers of apoptosis including Bcl-2, Bax.
- Markers of proliferation rate, such as Ki67.
- TP53 variant or expression.
- p27.
- E-cadherin.
- Microvessel density.
- DNA ploidy.
- p16.
- PTEN gene hypermethylation and allelic losses.
However, none of these has been prospectively validated, and they are not a part of the routine management of patients.
Clinical Presentation
In the United States, most prostate cancers are diagnosed as a result of screening; therefore, symptoms of cancer are infrequent at the time of diagnosis.[
- Decreased urinary stream.
- Urgency.
- Hesitancy.
- Nocturia.
- Incomplete bladder emptying.
These symptoms are nonspecific and more indicative of benign prostatic hyperplasia than cancer.
Although rare in the current era of widespread screening, prostate cancer may also present with symptoms of metastases, including bone pain, pathological fractures, or symptoms caused by bone marrow involvement.
Diagnostic Evaluation
Needle biopsy is the most common method used to diagnose prostate cancer. Most urologists now perform a transrectal biopsy using a bioptic gun with ultrasound guidance. Less frequently, a transperineal ultrasound-guided approach can be used in patients who may be at increased risk of complications from a transrectal approach.[
The use of magnetic resonance imaging (MRI)−directed biopsy in the initial diagnostic evaluation of prostate cancer is also being studied, either as a replacement for, or in addition to, standard systematic prostate needle biopsies. The data have been reported primarily by experienced MRI radiologists and urologists in referral centers, and generalizability of results is uncertain. A multicenter randomized trial of 500 patients has shown that, in experienced hands, a multiparametric MRI-directed biopsy is more accurate than a transrectal-guided biopsy to detect clinically significant cancers. MRI led to the detection of more Gleason score (≥7) lesions and fewer Gleason score (<7) lesions, with fewer biopsies overall.[
Prophylactic antibiotics, especially fluoroquinolones, are often used before transrectal needle biopsies. There are reports of increasing rates of sepsis, particularly with fluoroquinolone-resistant Escherichia coli, and hospitalization after the procedure.[
Prognostic Factors
The following factors influence the survival of patients with prostate cancer:[
-
Extent of tumor . -
Histological grade of tumor . -
Patient's age and health . -
Prostate-specific antigen (PSA) level .
Extent of tumor
When the cancer is confined to the prostate gland, long-term prognosis is excellent. Locally advanced cancer is not usually curable, but 5-year survival is still very good. If prostate cancer has spread to distant organs, current therapy will not cure it. Median survival is usually 1 to 3 years, and most of these patients will die of prostate cancer. Even in this group of patients, indolent clinical courses lasting for many years may be observed.
Histological grade of tumor
Poorly differentiated tumors are more likely to have metastasized before diagnosis and are associated with a poorer prognosis. The most commonly used method to report tumor differentiation is the Gleason score. For more information, see the
Patient's age and health
Any benefits of definitive local therapy with curative intent may take years to emerge. Therefore, therapy with curative intent is usually reserved for men with a sufficiently long life expectancy. For example, radical prostatectomy is often reserved for men with an estimated life expectancy of at least 10 years.
Prostate-specific antigen (PSA) level
PSA, an organ-specific marker, is often used as a tumor marker.[
For example, baseline PSA and rate of PSA change were associated with subsequent metastasis or prostate cancer death in a cohort of 267 men with clinically localized prostate cancer who were managed by watchful waiting or active surveillance in the control arm of a randomized trial comparing radical prostatectomy with watchful waiting or active surveillance.[
Serum acid phosphatase levels
Elevations of serum acid phosphatase are associated with poor prognosis in both localized and disseminated disease. However, serum acid phosphatase levels are not incorporated into the American Joint Committee on Cancer's staging system for prostate cancer.[
Use of nomograms as a prognostic tool
Several nomograms have been developed to predict outcomes either before radical prostatectomy [
Postoperative nomograms add pathological findings, such as capsular invasion, surgical margins, seminal vesicle invasion, and lymph node involvement. The nomograms, however, were developed at academic centers and may not be as accurate when generalized to nonacademic hospitals, where most patients are treated.[
Follow-Up After Treatment
The optimal follow-up strategy for men treated for prostate cancer is uncertain. Men should be interviewed and examined for symptoms or signs of recurrent or progressing disease, as well as side effects of therapy that can be managed by changes in therapy. However, using surrogate end points for clinical decision-making is controversial, and the evidence that changing therapy based on such end points translates into clinical benefit is weak. Often, rates of PSA change are thought to be markers of tumor progression. However, even though a tumor marker or characteristic may be consistently associated with a high risk of prostate cancer progression or death, it may be a poor predictor and of limited utility in making therapeutic decisions.
Although the PSA test is nearly universally used to follow patients, the diversity of recommendations on follow-up care reflects the lack of research evidence on which to base firm conclusions. A systematic review of international guidelines highlights the need for robust primary research to inform future evidence-based models of follow-up care for men with prostate cancer.[
Preliminary data from a retrospective cohort of 8,669 patients with clinically localized prostate cancer treated with either radical prostatectomy or radiation therapy suggested that short posttreatment PSA doubling time (<3 months in this study) fulfills some criteria as a surrogate end point for all-cause mortality and prostate cancer-specific mortality after surgery or radiation therapy.[
Likewise, a retrospective analysis (SWOG-S9916 [NCT00004001]) showed PSA declines of 20% to 40% (but not 50%) at 3 months and 30% or more at 2 months after initiation of chemotherapy for hormone-independent prostate cancer, and fulfilled several criteria of surrogacy for overall survival (OS).[
These observations should be independently confirmed in prospective study designs and may not apply to patients treated with hormonal therapy. In addition, there are no standardized criteria of surrogacy or standardized cut points for adequacy of surrogate end points, even in prospective trials.[
Follow-up after radical prostatectomy
After radical prostatectomy, a detectable PSA level identifies patients at elevated risk of local treatment failure or metastatic disease;[
For example, in a retrospective analysis of nearly 2,000 men who had undergone radical prostatectomy with curative intent and were followed for a mean of 5.3 years, 315 men (15%) demonstrated an abnormal PSA of 0.2 ng/mL or higher, which is considered evidence of biochemical recurrence. Among these 315 men, 103 (34%) developed clinical evidence of recurrence. The median time to the development of clinical metastasis after biochemical recurrence was 8 years. After the men developed metastatic disease, the median time to death was an additional 5 years.[
Follow-up after radiation therapy
For patients treated with radiation therapy, the combination of clinical tumor stage, Gleason score, and pretreatment PSA level is often used to estimate the risk of relapse.[
Follow-up after hormonal therapy
After hormonal therapy, reduction of PSA to undetectable levels provides information regarding the duration of progression-free status; however, decreases in PSA of less than 80% may not be predictive.[
References:
- National Cancer Institute: SEER Stat Fact Sheets: Prostate. Bethesda, Md: National Cancer Institute.
Available online . Last accessed October 22, 2024. - American Cancer Society: Cancer Facts and Figures 2025. American Cancer Society, 2025.
Available online . Last accessed January 16, 2025. - Lu-Yao GL, Albertsen PC, Moore DF, et al.: Outcomes of localized prostate cancer following conservative management. JAMA 302 (11): 1202-9, 2009.
- Albertsen PC, Moore DF, Shih W, et al.: Impact of comorbidity on survival among men with localized prostate cancer. J Clin Oncol 29 (10): 1335-41, 2011.
- Welch HG, Albertsen PC: Prostate cancer diagnosis and treatment after the introduction of prostate-specific antigen screening: 1986-2005. J Natl Cancer Inst 101 (19): 1325-9, 2009.
- Welch HG, Black WC: Overdiagnosis in cancer. J Natl Cancer Inst 102 (9): 605-13, 2010.
- Zlotta AR, Egawa S, Pushkar D, et al.: Prevalence of prostate cancer on autopsy: cross-sectional study on unscreened Caucasian and Asian men. J Natl Cancer Inst 105 (14): 1050-8, 2013.
- Helgesen F, Holmberg L, Johansson JE, et al.: Trends in prostate cancer survival in Sweden, 1960 through 1988: evidence of increasing diagnosis of nonlethal tumors. J Natl Cancer Inst 88 (17): 1216-21, 1996.
- Berner A, Harvei S, Skjorten FJ: Follow-up of localized prostate cancer, with emphasis on previous undiagnosed incidental cancer. BJU Int 83 (1): 47-52, 1999.
- Garnick MB: Prostate cancer: screening, diagnosis, and management. Ann Intern Med 118 (10): 804-18, 1993.
- Croswell JM, Kramer BS, Crawford ED: Screening for prostate cancer with PSA testing: current status and future directions. Oncology (Williston Park) 25 (6): 452-60, 463, 2011.
- Bill-Axelson A, Holmberg L, Ruutu M, et al.: Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 352 (19): 1977-84, 2005.
- Wilt TJ, Brawer MK, Jones KM, et al.: Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med 367 (3): 203-13, 2012.
- Hegarty J, Beirne PV, Walsh E, et al.: Radical prostatectomy versus watchful waiting for prostate cancer. Cochrane Database Syst Rev (11): CD006590, 2010.
- Andriole GL, Grubb RL, Buys SS, et al.: Mortality results from a randomized prostate-cancer screening trial. N Engl J Med 360 (13): 1310-9, 2009.
- Schröder FH, Hugosson J, Roobol MJ, et al.: Screening and prostate-cancer mortality in a randomized European study. N Engl J Med 360 (13): 1320-8, 2009.
- Sandblom G, Varenhorst E, Rosell J, et al.: Randomised prostate cancer screening trial: 20 year follow-up. BMJ 342: d1539, 2011.
- Djulbegovic M, Beyth RJ, Neuberger MM, et al.: Screening for prostate cancer: systematic review and meta-analysis of randomised controlled trials. BMJ 341: c4543, 2010.
- Ilic D, O'Connor D, Green S, et al.: Screening for prostate cancer: an updated Cochrane systematic review. BJU Int 107 (6): 882-91, 2011.
- Nelson WG, De Marzo AM, Isaacs WB: Prostate cancer. N Engl J Med 349 (4): 366-81, 2003.
- Zelefsky MJ, Eastham JA, Sartor AO: Cancer of the prostate. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Lippincott Williams & Wilkins, 2011, pp 1220-71.
- Chan TY, Partin AW, Walsh PC, et al.: Prognostic significance of Gleason score 3+4 versus Gleason score 4+3 tumor at radical prostatectomy. Urology 56 (5): 823-7, 2000.
- Albertsen PC, Hanley JA, Barrows GH, et al.: Prostate cancer and the Will Rogers phenomenon. J Natl Cancer Inst 97 (17): 1248-53, 2005.
- Thompson IM, Canby-Hagino E, Lucia MS: Stage migration and grade inflation in prostate cancer: Will Rogers meets Garrison Keillor. J Natl Cancer Inst 97 (17): 1236-7, 2005.
- Webb JA, Shanmuganathan K, McLean A: Complications of ultrasound-guided transperineal prostate biopsy. A prospective study. Br J Urol 72 (5 Pt 2): 775-7, 1993.
- Kasivisvanathan V, Rannikko AS, Borghi M, et al.: MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N Engl J Med 378 (19): 1767-1777, 2018.
- Ahdoot M, Wilbur AR, Reese SE, et al.: MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N Engl J Med 382 (10): 917-928, 2020.
- Nam RK, Saskin R, Lee Y, et al.: Increasing hospital admission rates for urological complications after transrectal ultrasound guided prostate biopsy. J Urol 183 (3): 963-8, 2010.
- Liss MA, Chang A, Santos R, et al.: Prevalence and significance of fluoroquinolone resistant Escherichia coli in patients undergoing transrectal ultrasound guided prostate needle biopsy. J Urol 185 (4): 1283-8, 2011.
- Gittes RF: Carcinoma of the prostate. N Engl J Med 324 (4): 236-45, 1991.
- Paulson DF, Moul JW, Walther PJ: Radical prostatectomy for clinical stage T1-2N0M0 prostatic adenocarcinoma: long-term results. J Urol 144 (5): 1180-4, 1990.
- Matzkin H, Eber P, Todd B, et al.: Prognostic significance of changes in prostate-specific markers after endocrine treatment of stage D2 prostatic cancer. Cancer 70 (9): 2302-9, 1992.
- Pisansky TM, Cha SS, Earle JD, et al.: Prostate-specific antigen as a pretherapy prognostic factor in patients treated with radiation therapy for clinically localized prostate cancer. J Clin Oncol 11 (11): 2158-66, 1993.
- Chodak GW, Thisted RA, Gerber GS, et al.: Results of conservative management of clinically localized prostate cancer. N Engl J Med 330 (4): 242-8, 1994.
- Carlton JC, Zagars GK, Oswald MJ: The role of serum prostatic acid phosphatase in the management of adenocarcinoma of the prostate with radiotherapy. Int J Radiat Oncol Biol Phys 19 (6): 1383-8, 1990.
- Stamey TA, Yang N, Hay AR, et al.: Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N Engl J Med 317 (15): 909-16, 1987.
- Stamey TA, Kabalin JN: Prostate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. I. Untreated patients. J Urol 141 (5): 1070-5, 1989.
- Stamey TA, Kabalin JN, McNeal JE, et al.: Prostate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. II. Radical prostatectomy treated patients. J Urol 141 (5): 1076-83, 1989.
- Stamey TA, Kabalin JN, Ferrari M: Prostate specific antigen in the diagnosis and treatment of adenocarcinoma of the prostate. III. Radiation treated patients. J Urol 141 (5): 1084-7, 1989.
- Andriole GL: Serum prostate-specific antigen: the most useful tumor marker. J Clin Oncol 10 (8): 1205-7, 1992.
- Fall K, Garmo H, Andrén O, et al.: Prostate-specific antigen levels as a predictor of lethal prostate cancer. J Natl Cancer Inst 99 (7): 526-32, 2007.
- Parekh DJ, Ankerst DP, Thompson IM: Prostate-specific antigen levels, prostate-specific antigen kinetics, and prostate cancer prognosis: a tocsin calling for prospective studies. J Natl Cancer Inst 99 (7): 496-7, 2007.
- Partin AW, Kattan MW, Subong EN, et al.: Combination of prostate-specific antigen, clinical stage, and Gleason score to predict pathological stage of localized prostate cancer. A multi-institutional update. JAMA 277 (18): 1445-51, 1997.
- Partin AW, Mangold LA, Lamm DM, et al.: Contemporary update of prostate cancer staging nomograms (Partin Tables) for the new millennium. Urology 58 (6): 843-8, 2001.
- Kattan MW, Eastham JA, Stapleton AM, et al.: A preoperative nomogram for disease recurrence following radical prostatectomy for prostate cancer. J Natl Cancer Inst 90 (10): 766-71, 1998.
- Stephenson AJ, Scardino PT, Eastham JA, et al.: Preoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Natl Cancer Inst 98 (10): 715-7, 2006.
- Kattan MW, Wheeler TM, Scardino PT: Postoperative nomogram for disease recurrence after radical prostatectomy for prostate cancer. J Clin Oncol 17 (5): 1499-507, 1999.
- Stephenson AJ, Scardino PT, Eastham JA, et al.: Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J Clin Oncol 23 (28): 7005-12, 2005.
- Shariat SF, Walz J, Roehrborn CG, et al.: External validation of a biomarker-based preoperative nomogram predicts biochemical recurrence after radical prostatectomy. J Clin Oncol 26 (9): 1526-31, 2008.
- Kattan MW, Shariat SF, Andrews B, et al.: The addition of interleukin-6 soluble receptor and transforming growth factor beta1 improves a preoperative nomogram for predicting biochemical progression in patients with clinically localized prostate cancer. J Clin Oncol 21 (19): 3573-9, 2003.
- Penson DF, Grossfeld GD, Li YP, et al.: How well does the Partin nomogram predict pathological stage after radical prostatectomy in a community based population? Results of the cancer of the prostate strategic urological research endeavor. J Urol 167 (4): 1653-7; discussion 1657-8, 2002.
- Greene KL, Meng MV, Elkin EP, et al.: Validation of the Kattan preoperative nomogram for prostate cancer recurrence using a community based cohort: results from cancer of the prostate strategic urological research endeavor (capsure). J Urol 171 (6 Pt 1): 2255-9, 2004.
- McIntosh HM, Neal RD, Rose P, et al.: Follow-up care for men with prostate cancer and the role of primary care: a systematic review of international guidelines. Br J Cancer 100 (12): 1852-60, 2009.
- D'Amico AV, Moul JW, Carroll PR, et al.: Surrogate end point for prostate cancer-specific mortality after radical prostatectomy or radiation therapy. J Natl Cancer Inst 95 (18): 1376-83, 2003.
- Petrylak DP, Ankerst DP, Jiang CS, et al.: Evaluation of prostate-specific antigen declines for surrogacy in patients treated on SWOG 99-16. J Natl Cancer Inst 98 (8): 516-21, 2006.
- Baker SG: Surrogate endpoints: wishful thinking or reality? J Natl Cancer Inst 98 (8): 502-3, 2006.
- Frazier HA, Robertson JE, Humphrey PA, et al.: Is prostate specific antigen of clinical importance in evaluating outcome after radical prostatectomy. J Urol 149 (3): 516-8, 1993.
- Pound CR, Partin AW, Eisenberger MA, et al.: Natural history of progression after PSA elevation following radical prostatectomy. JAMA 281 (17): 1591-7, 1999.
- Pisansky TM, Kahn MJ, Rasp GM, et al.: A multiple prognostic index predictive of disease outcome after irradiation for clinically localized prostate carcinoma. Cancer 79 (2): 337-44, 1997.
- Consensus statement: guidelines for PSA following radiation therapy. American Society for Therapeutic Radiology and Oncology Consensus Panel. Int J Radiat Oncol Biol Phys 37 (5): 1035-41, 1997.
- Roach M, Hanks G, Thames H, et al.: Defining biochemical failure following radiotherapy with or without hormonal therapy in men with clinically localized prostate cancer: recommendations of the RTOG-ASTRO Phoenix Consensus Conference. Int J Radiat Oncol Biol Phys 65 (4): 965-74, 2006.
- Kuban DA, el-Mahdi AM, Schellhammer PF: Prostate-specific antigen for pretreatment prediction and posttreatment evaluation of outcome after definitive irradiation for prostate cancer. Int J Radiat Oncol Biol Phys 32 (2): 307-16, 1995.
- Sandler HM, Dunn RL, McLaughlin PW, et al.: Overall survival after prostate-specific-antigen-detected recurrence following conformal radiation therapy. Int J Radiat Oncol Biol Phys 48 (3): 629-33, 2000.
- Ruckle HC, Klee GG, Oesterling JE: Prostate-specific antigen: concepts for staging prostate cancer and monitoring response to therapy. Mayo Clin Proc 69 (1): 69-79, 1994.
Stage Information for Prostate Cancer
Staging Tests
Most men are diagnosed with prostate cancer at an early clinical stage and do not have detectable metastases. They generally do not have to undergo staging tests, such as a bone scan, computed tomography (CT), or magnetic resonance imaging (MRI). However, staging studies are done if there is clinical suspicion of metastasis, such as bone pain, local tumor spread beyond the prostate capsule, or a substantial risk of metastasis (prostate-specific antigen [PSA] >20 ng/mL and Gleason score >7).[
Tests used to stage prostate cancer include:
-
Serum PSA level . -
MRI . -
Positron emission tomography (PET) .Gallium Ga 68 (68Ga)-gozetotide and fluorine F 18 (18F)-piflufolastat PET-CT .Fluorine F 18 (18F)-fluciclovine PET-CT .
-
Pelvic lymph node dissection (PLND) . -
Transrectal or transperineal biopsy . -
Transrectal ultrasound (TRUS) . -
CT scans . -
Technetium Tc 99m (99mTc)-methylene diphosphonate (MDP) bone scan .
Serum PSA level
Serum PSA can predict the results of radionuclide bone scans in newly diagnosed patients.
- In one series, only 2 of 852 patients (0.23%) with a PSA of less than 20 ng/mL had a positive bone scan in the absence of bone pain.[
2 ] - In another series of 265 patients with prostate cancer, 0 of 23 patients with a PSA of less than 4 ng/mL had a positive bone scan, and 2 of 114 patients with a PSA of less than 10 ng/mL had a positive bone scan.[
3 ]
Magnetic resonance imaging (MRI)
Although MRI has been used to detect extracapsular extension of prostate cancer, a positive-predictive value of about 70% and considerable interobserver variation are problems that make its routine use in staging uncertain.[
MRI is more sensitive than radionuclide bone scans in the detection of bone metastases, but it is impractical for evaluating the entire skeletal system.
Positron emission tomography (PET)
It is becoming more common to use PET-CT with specific radionuclide tracers to stage prostate cancer. Several tracers have been tested and shown the ability to detect either lymph node or distant metastases in certain patients with prostate cancer.
68Ga-gozetotide and 18F-piflufolastat PET-CT
Prostate-specific membrane antigen (PSMA) is a transmembrane receptor expressed in high levels in prostate cancer. PSMA can be targeted for imaging with 68Ga-gozetotide and 18F-piflufolastat. These radionuclide tracers have been tested for the imaging of nodes and metastases in the initial staging of intermediate- and high-risk prostate cancer, as well as imaging of suspected posttreatment recurrent disease in patients with an elevated PSA.
A phase III trial included 764 patients with intermediate- or high-risk prostate cancer who underwent 68Ga-gozetotide PET-CT staging. The trial reported a sensitivity of 40% and a specificity of 95% in the detection of nodal disease as compared with PLND.[
68Ga-gozetotide PET-CT was studied alongside CT and bone scan for the detection of metastatic disease in men with high-risk prostate cancer. Compared with conventional imaging, 68Ga-gozetotide PET-CT provided increased sensitivity (85% vs. 38%) and specificity (98% vs. 91%).[
18F-piflufolastat PET-CT had a sensitivity of 40% and a specificity of 98% in staging intermediate- or high-risk prostate cancer compared with PLND.[
Based on these data, the U.S. Food and Drug Administration (FDA) approved 68Ga-gozetotide and 18F-piflufolastat PET-CT for the initial staging of patients with prostate cancer and suspicion of metastatic disease, and for the evaluation of potential recurrence based on an elevated posttreatment PSA.[
18F-fluciclovine PET-CT
18F-fluciclovine PET-CT showed low sensitivity but high specificity in the initial lymph nodal staging of intermediate- and high-risk prostate cancer, compared with PLND.[
18F-fluciclovine also detected more bone metastases and was more sensitive and specific than 99mTc-MDP bone scan.[
The FDA approved 18F-fluciclovine PET-CT for the assessment of suspected recurrent disease in men with a rising posttreatment PSA.
Pelvic lymph node dissection (PLND)
PLND remains the most accurate method to assess metastasis to the pelvic nodes, and laparoscopic PLND has been shown to accurately assess pelvic nodes as effectively as an open procedure.[
The determining factor in deciding whether any type of PLND is indicated is when definitive therapy may be altered. For example, radical prostatectomy is generally reserved for men without lymph node metastasis. Likewise, preoperative seminal vesicle biopsy may be useful in patients with palpable nodules who are being considered for radical prostatectomy (unless they have a low Gleason score) because seminal vesicle involvement could affect the choice of primary therapy and predicts for pelvic lymph node metastasis.[
In patients with clinically localized (stage I or stage II) prostate cancer, Gleason pathological grade and enzymatic serum prostatic acid phosphatase values (even within normal range) predict the likelihood of capsular penetration, seminal vesicle invasion, or regional lymph node involvement.[
Having all patients undergo a PLND is debatable, but in patients undergoing a radical retropubic prostatectomy, nodal status is usually ascertained as a matter of course. Evidence is mounting that PLND is likely unnecessary in patients with a PSA less than 20 ng/mL and a low Gleason score who are undergoing radical perineal prostatectomy. This is especially true for patients whose malignancy was not palpable but detected on ultrasound.[
Transrectal or transperineal biopsy
The most common means to establish a diagnosis and determine the Gleason score in cases of suspected prostate cancer is by needle biopsy. Most urologists now perform a transrectal biopsy using a bioptic gun with ultrasound guidance. Less frequently, a transperineal ultrasound-guided approach can be used for those patients who may be at increased risk of complications from a transrectal approach.[
Transrectal ultrasound (TRUS)
TRUS may facilitate diagnosis by directing needle biopsy; however, ultrasound is operator dependent and does not assess lymph node size.
A prospective multi-institutional study of preoperative TRUS in men with clinically localized prostate cancer eligible for radical prostatectomy showed that TRUS was no better than digital rectal examination in predicting extracapsular tumor extension or seminal vesicle involvement.[
Computed tomography (CT) scans
CT scans can detect grossly enlarged lymph nodes but poorly define intraprostatic features;[
Technetium Tc 99m (99mTc)-methylene diphosphonate (MDP) bone scan
A 99mTc-MDP bone scan is the most widely used test for metastasis to the bone, which is the most common site of distant tumor spread.
Staging Systems
Historically, two systems have been in common use for the staging of prostate cancer.
- In 1975, the Jewett system (stage A through stage D) was described and has since been modified.[
25 ] This staging system is no longer in common use, but older studies and publications may refer to it. - In 1997, the American Joint Committee on Cancer (AJCC) and the International Union Against Cancer adopted a revised TNM (tumor, node, metastasis) system, which used the same broad T-stage categories as the Jewett system but included subcategories of T stage, such as a stage to describe patients diagnosed through PSA screening. This revised TNM system more precisely stratifies newly diagnosed patients.
AJCC Stage Groupings and TNM Definitions
The AJCC has designated staging by TNM classification.[
| Grade Group | Gleason Score | Gleason Pattern |
|---|---|---|
| a Adapted from AJCC: Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 715–26. | ||
| 1 | ≤6 | ≤3+3 |
| 2 | 7 | 3+4 |
| 3 | 7 | 4+3 |
| 4 | 8 | 4+4, 3+5, or 5+3 |
| 5 | 9 or 10 | 4+5, 5+4, or 5+5 |
| Stage | TNM | Descriptionb,c,d,e | PSAf | Gleason Score; Gleason Pattern (Grade Group)g | Illustration |
|---|---|---|---|---|---|
| T = primary tumor; N = regional lymph nodes; M = distant metastasis; cT = clinical T; PSA = prostate-specific antigen; pT = pathological T. | |||||
| a Adapted from AJCC: Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 715–26. | |||||
| The explanations for superscripts b through g are at the end of |
|||||
| I | cT1a–c, cT2a, N0, M0 | cT1 = Clinically inapparent tumor that is not palpable. | <10 | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | 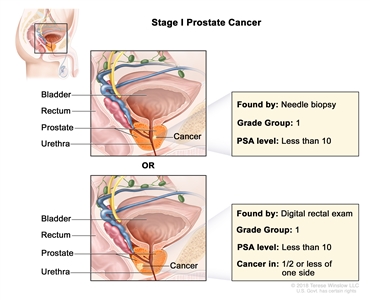 |
| –cT1a = Tumor incidental histological finding in ≤5% of tissue resected. | |||||
| –cT1b = Tumor incidental histological finding in >5% of tissue resected. | |||||
| –cT1c = Tumor identified by needle biopsy found in one or both sides, but not palpable. | |||||
| cT2 = Tumor is palpable and confined within prostate. | |||||
| –cT2a = Tumor involves ½ of one side or less. | |||||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| pT2, N0, M0 | pT2 = Organ confined. | <10 | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | ||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| Stage | TNM | Descriptionb,c,d,e | PSAf | Gleason Score; Gleason Pattern (Grade Group)g | Illustration |
|---|---|---|---|---|---|
| T = primary tumor; N = regional lymph nodes; M = distant metastasis; cT = clinical T; PSA = prostate-specific antigen; pT = pathological T. | |||||
| a Adapted from AJCC: Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 715–26. | |||||
| The explanations for superscripts b through g are at the end of |
|||||
| IIA | cT1a–c, cT2a, pT2, N0, M0 | See cT1a–c, cT2a descriptions in |
≥10 <20 | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | 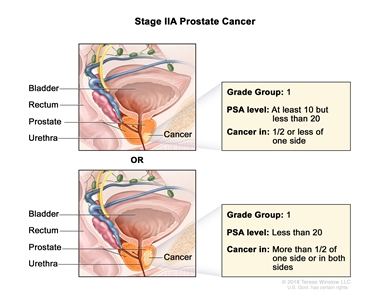 |
| pT2 = Organ confined. | |||||
| cT2b–c, N0, M0 | cT2 = Tumor is palpable and confined within prostate. | <20 | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | ||
| cT2b = Tumor involves >½ of one side but not both sides. | |||||
| cT2c = Tumor involves both sides. | |||||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| IIB | T1–2, N0, M0 | T1 = Clinically inapparent tumor that is not palpable. | <20 | Gleason Score, 7; Gleason Pattern 3+4 (2). | 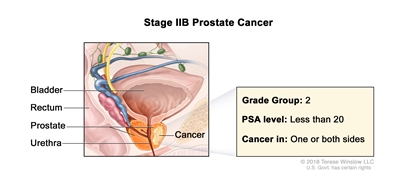 |
| –T1a = Tumor incidental histological finding in ≤5% of tissue resected. | |||||
| –T1b = Tumor incidental histological finding in >5% of tissue resected. | |||||
| –T1c = Tumor identified by needle biopsy found in one or both sides, but not palpable. | |||||
| cT2 = Tumor is palpable and confined within prostate. | |||||
| –cT2a = Tumor involves ½ of one side or less. | |||||
| –cT2b = Tumor involves >½ of one side but not both sides. | |||||
| –cT2c = Tumor involves both sides. | |||||
| pT2 = Organ confined. | |||||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| IIC | T1–2, N0, M0 | See T1–2, N0, M0 descriptions above in Stage IIB. | <20 | Gleason Score, 7; Gleason Pattern, 4 + 3 (3). |  |
| T1–2, N0, M0 | See T1–2, N0, M0 descriptions above in Stage IIB. | <20 | Gleason Score, 8; Gleason Pattern, 4+4, 3+5, or 5+3 (4). | ||
| Stage | TNM | Descriptionb,c,d,e | PSAf | Gleason Score; Gleason Pattern (Grade Group)g | Illustration |
|---|---|---|---|---|---|
| T = primary tumor; N = regional lymph nodes; M = distant metastasis; cT = clinical T; PSA = prostate-specific antigen; pT = pathological T. | |||||
| a Adapted from AJCC: Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 715–26. | |||||
| The explanations for superscripts b through g are at the end of |
|||||
| IIIA | T1–2, N0, M0 | See T1–2, N0, M0 descriptions in |
≥20 | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | 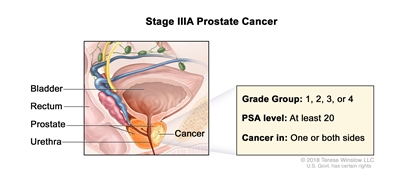 |
| Gleason Score, 7; Gleason Pattern 3+4 (2). | |||||
| Gleason Score, 7; Gleason Pattern, 4+3 (3). | |||||
| Gleason Score, 8; Gleason Pattern, 4+4, 3+5, or 5+3 (4). | |||||
| IIIB | T3–4, N0, M0 | cT3 = Extraprostatic tumor that is not fixed or does not invade adjacent structures. | Any value | Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | 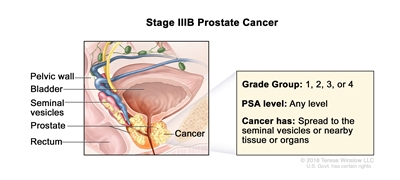 |
| –cT3a = Extraprostatic extension (unilateral or bilateral). | Gleason Score, 7; Gleason Pattern 3+4 (2). | ||||
| –cT3b = Tumor invades seminal vesicle(s). | Gleason Score, 7; Gleason Pattern, 4+3 (3). | ||||
| pT3 = Extraprostatic extension. | Gleason Score, 8; Gleason Pattern, 4+4, 3+5, or 5+3 (4). | ||||
| –pT3a = Extraprostatic extension (unilateral or bilateral) or microscopic invasion of bladder neck. | |||||
| –pT3b = Tumor invades seminal vesicle(s). | |||||
| cT4 or pT4= Tumor is fixed or invades adjacent structures other than seminal vesicles such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall. | |||||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| IIIC | Any T, N0, M0 | TX = Primary tumor cannot be assessed. | Any value | Gleason Score, 9 or 10; Gleason Pattern, 4+5, 5+4, or 5+5 (5). | 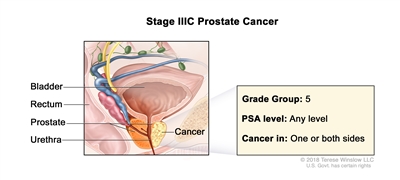 |
| T0 = No evidence of primary tumor. | |||||
| T1 = Clinically inapparent tumor that is not palpable. | |||||
| –T1a = Tumor incidental histological finding in ≤5% of tissue resected. | |||||
| –T1b = Tumor incidental histological finding in >5% of tissue resected. | |||||
| –T1c = Tumor identified by needle biopsy found in one or both sides, but not palpable. | |||||
| cT2 = Tumor is palpable and confined within prostate. | |||||
| –cT2a = Tumor involves ½ of one side or less. | |||||
| –cT2b = Tumor involves >½ of one side but not both sides. | |||||
| –cT2c = Tumor involves both sides. | |||||
| –pT2 = Organ confined. | |||||
| cT3 = Extraprostatic tumor that is not fixed or does not invade adjacent structures. | |||||
| –cT3a = Extraprostatic extension (unilateral or bilateral). | |||||
| –cT3b = Tumor invades seminal vesicle(s). | |||||
| pT3 = Extraprostatic extension. | |||||
| –pT3a = Extraprostatic extension (unilateral or bilateral) or microscopic invasion of bladder neck. | |||||
| –pT3b = Tumor invades seminal vesicle(s). | |||||
| cT4 or pT4 = Tumor is fixed or invades adjacent structures other than seminal vesicles such as external sphincter, rectum, bladder, levator muscles, and/or pelvic wall. | |||||
| N0 = No positive regional nodes. | |||||
| M0 = No distant metastasis. | |||||
| Stage | TNM | Descriptionb,c,d,e | PSAf | Gleason Score; Gleason Pattern (Grade Group)g | Illustration |
|---|---|---|---|---|---|
| T = primary tumor; N = regional lymph nodes; M = distant metastasis; cT = clinical T; PSA = prostate-specific antigen; pT = pathological T. | |||||
| a Adapted from AJCC: Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.:AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer, 2017, pp. 715–26. | |||||
| b When either PSA or Grade Group is not available, grouping should be determined by T category and/or either PSA or Grade Group as available. | |||||
| c There is no pathological T1 classification. | |||||
| d Positive surgical margin should be indicated by an R1 descriptor, indicating residual microscopic disease. | |||||
| e When more than one site of metastasis is present, the most advanced category is used. M1c is most advanced. | |||||
| f PSA values are used to assign this category. | |||||
| g Recently the Gleason system has been compressed into so-called Grade Groups.[ |
|||||
| IVA | Any T, N1, M0 | Any T = See descriptions in |
See Any PSA values in |
Gleason Score, ≤6; Gleason Pattern, ≤3+3 (1). | 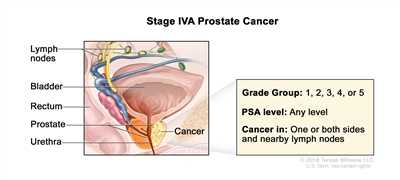 |
| Gleason Score, 7; Gleason Pattern 3+4 (2). | |||||
| Gleason Score, 7; Gleason Pattern, 4+3 (3). | |||||
| N1 = Metastases in regional node(s). | Gleason Score, 8; Gleason Pattern, 4+4, 3+5, or 5+3 (4). | ||||
| M0 = No distant metastasis. | Gleason Score, 9 or 10; Gleason Pattern, 4+5, 5+4, or 5+5 (5). | ||||
| IVB | Any T, Any N, M1 | Any T = See descriptions in |
See Any PSA values |
Any Gleason Score; Gleason Pattern (Grade Group) = See above in Stage IVA. | 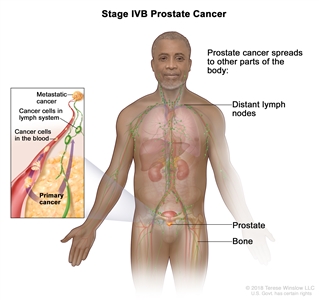 |
| NX = Regional nodes were not assessed. | |||||
| N0 = No positive regional nodes. | |||||
| N1 = Metastases in regional node(s). | |||||
| M1 = Distant metastasis. | |||||
| –M1a = Nonregional lymph node(s). | |||||
| –M1b = Bone(s). | |||||
| –M1c = Other site(s) with or without bone disease. | |||||
References:
- Zelefsky MJ, Eastham JA, Sartor AO: Cancer of the prostate. In: DeVita VT Jr, Lawrence TS, Rosenberg SA: Cancer: Principles and Practice of Oncology. 9th ed. Lippincott Williams & Wilkins, 2011, pp 1220-71.
- Oesterling JE, Martin SK, Bergstralh EJ, et al.: The use of prostate-specific antigen in staging patients with newly diagnosed prostate cancer. JAMA 269 (1): 57-60, 1993.
- Huncharek M, Muscat J: Serum prostate-specific antigen as a predictor of radiographic staging studies in newly diagnosed prostate cancer. Cancer Invest 13 (1): 31-5, 1995.
- Schiebler ML, Yankaskas BC, Tempany C, et al.: MR imaging in adenocarcinoma of the prostate: interobserver variation and efficacy for determining stage C disease. AJR Am J Roentgenol 158 (3): 559-62; discussion 563-4, 1992.
- Hope TA, Eiber M, Armstrong WR, et al.: Diagnostic Accuracy of 68Ga-PSMA-11 PET for Pelvic Nodal Metastasis Detection Prior to Radical Prostatectomy and Pelvic Lymph Node Dissection: A Multicenter Prospective Phase 3 Imaging Trial. JAMA Oncol 7 (11): 1635-1642, 2021.
- Hofman MS, Lawrentschuk N, Francis RJ, et al.: Prostate-specific membrane antigen PET-CT in patients with high-risk prostate cancer before curative-intent surgery or radiotherapy (proPSMA): a prospective, randomised, multicentre study. Lancet 395 (10231): 1208-1216, 2020.
- Fendler WP, Calais J, Eiber M, et al.: Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol 5 (6): 856-863, 2019.
- Calais J, Ceci F, Eiber M, et al.: 18F-fluciclovine PET-CT and 68Ga-PSMA-11 PET-CT in patients with early biochemical recurrence after prostatectomy: a prospective, single-centre, single-arm, comparative imaging trial. Lancet Oncol 20 (9): 1286-1294, 2019.
- Pienta KJ, Gorin MA, Rowe SP, et al.: A Phase 2/3 Prospective Multicenter Study of the Diagnostic Accuracy of Prostate Specific Membrane Antigen PET/CT with 18F-DCFPyL in Prostate Cancer Patients (OSPREY). J Urol 206 (1): 52-61, 2021.
- U.S. Food and Drug Administration: FDA approves first PSMA-targeted PET imaging drug for men with prostate cancer. Food and Drug Administration, 2020.
Available online . Last accessed February 13, 2025. - U.S. Food and Drug Administration: FDA approves second PSMA-targeted PET imaging drug for men with prostate cancer. Food and Drug Administration, 2021.
Available online . Last accessed February 13, 2025. - Selnæs KM, Krüger-Stokke B, Elschot M, et al.: 18F-Fluciclovine PET/MRI for preoperative lymph node staging in high-risk prostate cancer patients. Eur Radiol 28 (8): 3151-3159, 2018.
- Suzuki H, Jinnouchi S, Kaji Y, et al.: Diagnostic performance of 18F-fluciclovine PET/CT for regional lymph node metastases in patients with primary prostate cancer: a multicenter phase II clinical trial. Jpn J Clin Oncol 49 (9): 803-811, 2019.
- Alemozaffar M, Akintayo AA, Abiodun-Ojo OA, et al.: [18F]Fluciclovine Positron Emission Tomography/Computerized Tomography for Preoperative Staging in Patients with Intermediate to High Risk Primary Prostate Cancer. J Urol 204 (4): 734-740, 2020.
- Chen B, Wei P, Macapinlac HA, et al.: Comparison of 18F-Fluciclovine PET/CT and 99mTc-MDP bone scan in detection of bone metastasis in prostate cancer. Nucl Med Commun 40 (9): 940-946, 2019.
- Schuessler WW, Pharand D, Vancaillie TG: Laparoscopic standard pelvic node dissection for carcinoma of the prostate: is it accurate? J Urol 150 (3): 898-901, 1993.
- Stone NN, Stock RG, Unger P: Indications for seminal vesicle biopsy and laparoscopic pelvic lymph node dissection in men with localized carcinoma of the prostate. J Urol 154 (4): 1392-6, 1995.
- Oesterling JE, Brendler CB, Epstein JI, et al.: Correlation of clinical stage, serum prostatic acid phosphatase and preoperative Gleason grade with final pathological stage in 275 patients with clinically localized adenocarcinoma of the prostate. J Urol 138 (1): 92-8, 1987.
- Fournier GR, Narayan P: Re-evaluation of the need for pelvic lymphadenectomy in low grade prostate cancer. Br J Urol 72 (4): 484-8, 1993.
- Daniels GF, McNeal JE, Stamey TA: Predictive value of contralateral biopsies in unilaterally palpable prostate cancer. J Urol 147 (3 Pt 2): 870-4, 1992.
- Webb JA, Shanmuganathan K, McLean A: Complications of ultrasound-guided transperineal prostate biopsy. A prospective study. Br J Urol 72 (5 Pt 2): 775-7, 1993.
- Smith JA, Scardino PT, Resnick MI, et al.: Transrectal ultrasound versus digital rectal examination for the staging of carcinoma of the prostate: results of a prospective, multi-institutional trial. J Urol 157 (3): 902-6, 1997.
- Gerber GS, Goldberg R, Chodak GW: Local staging of prostate cancer by tumor volume, prostate-specific antigen, and transrectal ultrasound. Urology 40 (4): 311-6, 1992.
- Hanks GE, Krall JM, Pilepich MV, et al.: Comparison of pathologic and clinical evaluation of lymph nodes in prostate cancer: implications of RTOG data for patient management and trial design and stratification. Int J Radiat Oncol Biol Phys 23 (2): 293-8, 1992.
- Jewett HJ: The present status of radical prostatectomy for stages A and B prostatic cancer. Urol Clin North Am 2 (1): 105-24, 1975.
- Prostate. In: Amin MB, Edge SB, Greene FL, et al., eds.: AJCC Cancer Staging Manual. 8th ed. Springer; 2017, pp. 715–26.
- Epstein JI, Egevad L, Amin MB, et al.: The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: Definition of Grading Patterns and Proposal for a New Grading System. Am J Surg Pathol 40 (2): 244-52, 2016.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the
Healthwise, Healthwise for every health decision, and the Healthwise logo are trademarks of Ignite Healthwise, LLC.
Page Footer
I want to...
Audiences
Secure Member Sites
The Cigna Group Information
Disclaimer
Individual and family medical and dental insurance plans are insured by Cigna Health and Life Insurance Company (CHLIC), Cigna HealthCare of Arizona, Inc., Cigna HealthCare of Illinois, Inc., Cigna HealthCare of Georgia, Inc., Cigna HealthCare of North Carolina, Inc., Cigna HealthCare of South Carolina, Inc., and Cigna HealthCare of Texas, Inc. Group health insurance and health benefit plans are insured or administered by CHLIC, Connecticut General Life Insurance Company (CGLIC), or their affiliates (see
All insurance policies and group benefit plans contain exclusions and limitations. For availability, costs and complete details of coverage, contact a licensed agent or Cigna sales representative. This website is not intended for residents of New Mexico.